Introduction
In this final chapter on water we need to discuss what happens when this delicate balance of body fluids in terms of osmotic and hydrostatic pressure becomes disrupted by abnormal physiological conditions such as autoimmunity and prescription medicine causing Edema and Hyponatremia/Hypernatremia.
Body fluids ( Review)

The initial premise to appreciate between the fluids inside the cell ( Intracellular ) and the fluids outside of the cell ( extracellular ) is that if they are in osmotic equilibrium, which means that no movement of water between these environments will occur. Typically, the extracellular environment made up of plasma/interstitial fluid, and Intracellular fluid is basically regulated around a total osmotic pressure at 37 dg C of 5443, 5423 and 5423 measured in mm Hg respectively *. However, if small changes are made to either fluid concentration, a potentially large osmotic pressure can develop across the cell membrane. Let us review what we discussed in Part IX. The intracellular fluid ( inside) contains a high density of Potassium, Magnesium and Phosphate ions, while the extracellular fluid (ECF) (outside) contains a high density of Sodium, Chloride and Bicarbonate ions ( small quantities of potassium, magnesium, phosphate and organic acid ions are also contained in the ECF) and cell nutrients that include Oxygen, Glucose, Fatty acids, Amino acids and Carbon dioxide. This is the fluidic constituents of the cellular environment, which is shown in the diagram below. Extracellular fluid is transported throughout the entire body in the bloodstream in 2 steps, 1.The movement of blood in the blood vessels, 2. Fluid between the blood capillaries and into the intercellular space. As the blood circulates within the blood capillaries there is a continual exchange of extracellular fluid between the blood plasma and the interstitial fluid that fills the intercellular space. Interstitial fluid is located outside of the blood vessels and intravascular is fluid inside the blood vessels. However the capillary walls are permeable so the contents of the interstitial fluid and the intravascular fluid move in/out of the blood vessel by diffusion. So the extracellular fluid throughout the body continually mixes with both the intravascular and interstitial fluids. Interstitial fluid is made up of water solvent, sugars, salts (potassium, magnesium and phosphate as mentioned above) ,fatty acids,amino acids, coenzymes, hormones, neurotransmitters, white blood cells (immune system cells) and cell waste products; quite a biological soup, although its contents are variable depending upon the cell exchanges and biological tissue. In terms of body fluid volume:
Intracellular (Total fluid inside cells) = 25 litres
Extracellular (Total fluid Outside cells) = 15 litres
Interstitial (Total fluid outside of the blood vessels) = 12 litres
Intravascular( Total fluid inside of the blood vessels = 3 litres
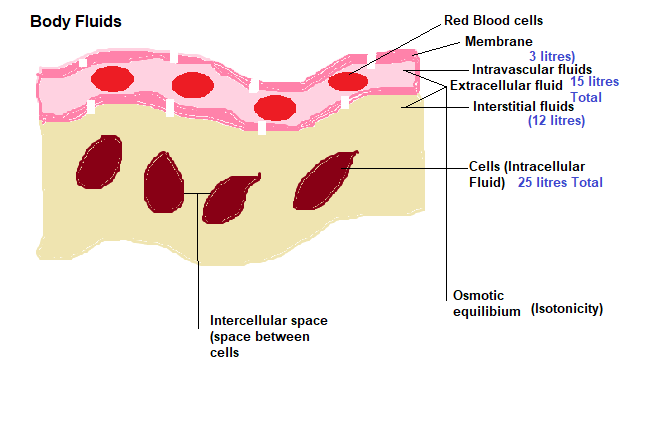
* This measurement is based on the different fluids if placed on one side of the cell membrane and pure water on the other
Osmosis review

Osmosis is the action of water diffusion across a semipermeable membrane that restricts solutes but allows water to flow from a high water concentration environment to a low water concentration environment. By adding solutes such as sodium chloride lowers water concentration, but still, whatever the solute concentration, it is the water concentration that will dictate the directional flow until equilibrium is achieved across both sides of the membrane. So by adding or removing solutes to water can change the water concentration, there is no longer equilibrium between the inside and the outside of the cell, osmotic pressure changes ( the higher the osmotic pressure, the lower the water concentration and the higher the solute concentration) and thus creates movement across the membrane by water diffusion. If equilibrium is maintained, the solutions on either side of the membrane have the same osmotic pressure, then it is said to be Isotonic. If, as we mentioned above the solutes change, especially the intracellular fluid, the 2 fluid environments are not in osmotic equilibrium, and the intracellular fluid has a lower solute concentration, it becomes a Hypotonic solution, where water will diffuse into the cell causing the cell to swell. If the intracellular solution has a higher concentration of solutes, then water will diffuse out of the cell making the fluid more concentrated and Hypertonic, causing severe hydration and the cell will shrink.
Why it is crucial to maintain osmotic equilibrium ?
So why am i explaining all this boring fluidic chemistry ?..because I think now you can appreciate how crucial it is to maintain the intracellular and extracellular fluid in balance. If you drink a glass of water, then momentarily osmotic equilibrium is disturbed but the body adjusts rapidly and it takes approximately 30 minutes to adjust the 100 trillion cells in the body..I know, as Dr B would say…WOW. Furthermore, this is one of the reasons why there exists this sophisticated feedback and sensing systems involving the Heart ( Barometric reflex), Adrenals (Aldosterone), Pituitary ( Antidiuretic hormone ADH), the Kidney ( Central fluid regulation) and the Hypothalamus/Medulla Oblongata ( Central system control ).
What can go wrong ?
Various reasons can cause a disruption in osmotic equilibrium, such as drinking water, dehydration, intravenous infusion of solutions, excessive loss of isotonic fluid from the GI Tract, profuse sweating, diarrhea, hemorrhage. As we mentioned in the last paragraph, drinking water only temporarily disrupts osmotic equilibrium giving the body time to rebalance the whole cellular population of the body. Intravenous infusion of fluid is a normal course of events by physicians to rehydrate dehydrated individuals. Generally these are isotonic saline solutions that simply increase extracellular fluid volume, since the solution is isotonic it will not trigger an osmotic effect, leaving sodium and chloride remaining in the extracellular environment. If the purpose is to drive more water out of the cells, than a hypertonic solution would be administered leaving the sodium and chloride unaltered, or a hypotonic solution would be used to drive water into the cells, until osmotic equilibrium has been attained. In this case, both fluid environments would increase, but the intracellular fluid volume would increase more. Excessive loss of isotonic fluid from the GI Tract is is largely due to diarrhea, and it is the loss of extracellular fluid ( plasma and interstitial) only, which could lead to a decrease in blood volume and blood pressure. Hemorrhaging is also a case of isotonic fluid loss resulting in an extracellular fluid loss and a decrease in cellular volume of the red blood cells only, so again isotonic loss does not cause any osmotic variance. As a result of a blood capillary pressure drop, the kidney is triggered to reabsorb interstitial fluid so both hematocrit (ratio of red blood cell volume to the total volume of blood) and plasma albumin ( the main protein of human blood plasma) concentration, decrease causing a drop in plasma oncotic pressure ( a form of osmotic pressure exerted by blood proteins), and once BP is restored this would result in a greater shift between extracellular fluid from the plasma to the volume of interstitial fluid. Sweating concerns a loss of hypertonic fluid since both water and solutes leave the body together and this will definitely trigger an osmotic action, since osmolality has increased, causing a movement of water from the intracellular space into the extracellular space.
Conventional medicine and causative mysticism

Syndrome of inappropriate antidiuretic hormone secretion (SIADH)
There exists other causes for body fluid volume disturbance, and one involves ‘excessive antidiuretic hormone ( ADH ) secretion which results in renal excretion of hypertonic urine. You may recall in the last article where in the case of excess sweating the osmoreceptors trigger the Pituitary gland to secrete a stored hormone Antidiuretic (ADH) that is sent to the kidney activating the collecting ducts to reabsorb more water thus preventing excess water loss through the urine. As we stated in the last paragraph, sweating is the loss of hypertonic fluid, so it is the plasma hypertonicity that activate these receptors. ADH secretion stimulates the cells lining the collection ducts in the kidney to reabsorb more water and transport it to the bloodstream, thus increasing blood volume and blood pressure to normal levels. In this abnormal condition hypertonic fluid depletion will cause a shift in plasma osmolarity where the intracellular solutes become diluted creating a hypotonic solution resulting in an inrush of water into the cell thus swelling the cell as mentioned above. Since excessive ADH is being released there is an unstoppable increase in solute free water being absorbed by the collecting ducts of the kidney causing a dilution of blood solutes and low sodium concentration/decreased volume in the extracellular fluid, a condition known as Hyponatremia, This condition can also be caused by diarrhea and vomiting, the overuse of diuretic drugs, and Addison’s disease an autoimmune condition that damages the adrenal gland impairing it to command the kidney to reabsorb sodium. Another condition exists known as Hypernatremia which is basically a state of hyperosmotic dehydration due to either loss of water or an excess of sodium ions in the extracellular fluid caused by the lack of ADH secretion and as a result the kidneys dump excess water that should be conserved, into the urinary tract as dilute urine (diabetes insipidus).
How can the pituitary secrete an excessive amount of ADH ?
According to the literature, Guillain – Barre syndrome is an autoimmune disease that affects the peripheral nervous system and in some, interference of the autonomic nervous system that cause abnormalities in heart rate and blood pressure. This makes sense since ADH will be secreted to adjust the BP to normal levels and it will continue to be secreted until the BP has reached normal levels which it won’t until the nervous system problem has been solved. According to the Mayo clinic, a well respected institution but they write on their website:
‘The exact cause of Guillain-Barre syndrome is unknown. But it is often preceded by an infectious illness such as a respiratory infection or the stomach flu. There’s no known cure for Guillain-Barre syndrome, but several treatments can ease symptoms and reduce the duration of the illness’.
However, we have discussed the causes and cures for autoimmune conditions at length in our article series ‘Autoimmune disease’ so we know the cause and we know how to cure it. This is the same prognosis for Addison’s disease that causes a decreased secretion of aldosterone impairing the kidney’s ability to reabsorb sodium.
https://www.extremehealthacademy.com/autoimmune-disease-part-1/
Various cancers according to Wikipedia can cause SIADH, so we know how to treat cancer and cure it from our articles ‘The anxiety of Wo(man) – Cancer:
Another cause according to wikipedia is Cystic Fibrosis(CF) that infects the lungs, but also can affect the pancreas, Liver, kidneys and intestines. They inform us that CF is inherited in an autosomal recessive manner which means that there are mutations in both copies of the gene that express a membrane protein/Chloride channel called Cystic fibrosis transmembrane conductance regulator (CFTR), that leads to dysregulation of epithelial fluid transport in the organs affected. This sounds like a convincing cause, but the chances of both gene copies being mutant is highly questionable, and besides Dr Joel Wallach proved in 1977 that CF is a congenital or neonatal deficiency of the trace mineral Selenium. He found by chance while working with 6 month old primates at the Yerkes primate center. The condition of CF in the rhesus monkeys could be replicated and his discovery from an autopsy taken on the monkey found pancreatic disease and bronchial mucus production. Dr Victor Nassar an Emory pediatric pathologist at Atlanta’s Grady Memorial hospital and Dr John Esterly a pathologist and national authority for CF at the Chicago’s Lying In Hospital both confirmed the diagnosis. Remember, contrary to the conventional medical belief of inherited mutagenicity, we are not victims of our genes because of the discovery of special DNA control regions that epigenetically control our genes, which is also discussed in the article series Epigenetics :
https://www.extremehealthacademy.com/the-basics-of-epigenetics-part-1/
Adrenal Problems
As we mentioned earlier Addison’s disease is a problem with the adrenal gland caused by the inappropriate functioning of the immune system, actually attacking the adrenal tissue as if it were foreign ( autoimmunity). In effect, it resembles adrenal burnout, or a hypoactive state where the adrenal is making insufficient hormone production leading to weight loss, pigmentation dysruption ( skin gets darker), excessive inflammation due to lack of cortisol ( the body’s anti inflammatory hormone) secretion, salt cravings and low potassium ( it is necessary to limit potassium temporarily until the problem is fixed ), but necessary to consume salt. This is also a reason that Hypernatremia occurs. On the other hand another reason for SIADH could be due to Cushing’s disease which is the opposite to Addison’s, since Cushing’s is where the adrenals are in a hyperstate and producing excessive amount of hormones, and the gland is low in potassium and high in salt (NaCl). To explain Cushing’s I would like to reserve this for a future article. Suffice to say Cushing’s syndrome can be caused by ingesting exogenous drugs such as steroids over a long period of time to treat autoimmune and inflammatory disorders, or endogenous cortisol production. In previous articles we described how the hypothalamus secretes corticotropin releasing hormone (CRH) to stimulate the pituitary gland to secrete Adrenocorticotropic hormone ( ACTH ) which then travel to the adrenal cortex, stimulating the cells in the zona fasciculata to produce cortisol, but in Cushing’s syndrome the cortisol levels are constantly high. One reason for this is pituitary Adenoma, a benign tumor tissue growth that develops on the pituitary causing an excess of ACTH production and an overstimulation of adrenal cortex producing excess cortisol.
Edema
This is a condition that manifests itself as swelling, located beneath the skin and in body cavities. This is a result of abnormal accumulation of fluid, generally in the extracellular fluid, but it can also affect the intracellular fluid. There can be various reasons tthat cause the accumulation of fluid in the extracellular environment, specifically in the interstitial space (outside of the blood vessels) by abnormal leakage from the blood capillaries, or the prevention of the lymphatic system from returning fluid from the interstitium back into the general circulation. Leakage from the capillaries occurs due to excess pressure caused by abnormal salt and water retention by a dysfunctional kidney, compromising salt and water excretion through the urinary tract. As a result these products leak out from the blood into the interstitial space increasing its volume and increasing BP, and erupting systemic edema. Kidney or liver (cirrhosis for example) problems, and malnutrition can decrease protein plasma concentration ( falling below 2.5 g/100ml), referred to as nephrotic syndrome, increasing capillary permeability thus causing edema. In addition, edema can develop from toxicity, bacterial infection, burns and vitamin deficiency (especially Vit C). Heart dysfunction such as high venous pressure ( Blockage ) and constriction, decrease of arteriolar resistance, excess body heat and sympathetic branch (Autonomic nervous system ANS) dysfunction can also induce edema. Finally, edema can arise from lymph return blockage due to cancer or infection. In essence most of these problems can boil down to a toxic/nutrient deficient lifestyle which you can correct and again I reference articles on the 90 essential nutrients and here is the link to the first article within the series of 17 articles:
https://www.extremehealthacademy.com/90-essential-nutrients-part-1-overview/
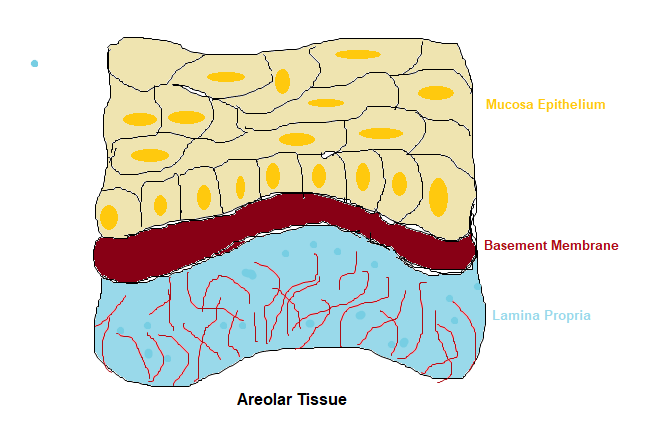
Generally, edema is an inflammatory issue that causes inflammation within the Areolar tissue. So what is areolar tissue, well as the name suggests areola means ‘small open space’ and it is the body’s universal packing and connecting tissue that cushions, protects and holds the organs together in their rightful position, like parcel bubble wrap but much more sophisticated. A soft connective tissue that underlies all mucous membranes ( such as the small intestines or skin for example) is areolar tissue called the Lamina Propria. This is made up of a fluid matrix of various fibers that form a loose network surrounded by an empty space ( areola ). This arrangement is shown in the diagram below. The Lamina Propria provides a reservoir of water and salts to support nutritionally, the surrounding tissue, where the cells pick up their required nutrients and eliminate their waste products into this tissue fluid. When this part of the body becomes inflamed this reservoir swells from additional fluid to which the areola tissue soaks up like a sponge.
Poisonous chemicals

One last note on the causes of SIADH, and that is the use of prescription drugs. According to Wikipedia ( and confirmed on drugs website rxlist.com) prescription medication that include Chlorpropamide (an antidiuretic used for diabetes insipidus, a form of diabetes that is sensitive to vasopressin or ADH) , Clofibrate ( used as for lowering lipids by promoting VLDL to LDL conversion), Phenothiazine ( antipsychotic drug to treat schizophrenia), Ifosfamide (Chemotherapy drug), Cyclophosphamide (Chemotherapy and immunosuppression drug), Carbamazepine (anticonvulsant), Oxcarbazepine (anticonvulsant) . Valproic acid (used to treat epilepsy and bipolar disorder), SSRI’s (antidepressant), Oxytocin ( hormone produced by the pituitary gland to stimulate uterine muscle contractions inducing labor), Vincristine (Chemotherapy drug), Morphine and Amitriptyline ( used to treat various depressive and anxiety disorders) can induce varied forms of SIADH, as well as the recreational drug Ecstasy.
Important note: In my articles I attempt to describe the body’s physiological processes so the reader can at least appreciate the complexity and precision of these various body processes and in doing so, respect these mechanisms by embracing a nutrient efficient/non toxic lifestyle to keep them running normally.. As I have said before..THE BODY DOES NOT CONTAIN THE ‘BLUEPRINTS’ TO EFFICIENTLY METABOLISE MAN MADE FOOD NOR MAN MADE PRESCRIPTION MEDICATION. Ignoring this will ultimately create physiological imbalance and organ/tissue damage and invite what is termed in the allopathic universe ‘DIS-EASE.
The body’s plumbing mechanics

I have to say that physicians have a lot to deal with when problems arise in their patient’s physiology, they not only need to be knowledgeable on human physiology, but they need to be aware of a certain amount of electrical and mechanical bioengineering that goes on in the body. To finalise our discussion on body fluid dysfunction I want to discuss Interstitial fluid hydrostatic pressure. What is this ?..The primary force that drives fluid between capillaries and tissues is hydrostatic pressure Blood capillary pressure (BCP), developed by blood pressure against the capillary wall, forces fluid from the capillaries and into the tissue, and when this happens the hydrostatic pressure in the interstitial fluid increases, referred to as Interstitial fluid hydrostatic pressure (IFHP). Since BCP is higher than IFHP, because the lymph system is continually absorbing excess fluid from the tissues, this fluid movement is referred to as Filtration. Previously we discussed osmotic pressure and it is this pressure that works in the opposite direction i.e moves fluid from the interstitial space back into the blood capillaries. In medicine, pressure is measured in millimetres of mercury (mm Hg), so the ‘perfect’ blood pressure in the eyes of allopathy is 120mm/ Hg. IFHP is generally at -3 mm Hg with an approx fluid volume of 12 litres in a gel like viscosity, meaning that the fluid is bound in a proteoglycan meshwork leaving no free fluid space, which is considered normal, and opposes further filtration into the tissues.
Ensure the normal flow of the lymphatic system
However, if IFHP increases to 0 or a positive value say + 3 mm HG, and the tissue ‘compliance (defined to be the ease that a blood vessel expands when filled with a volume of blood for example amounting to a change in volume divided by a change in pressure, where C = deltaV/delta P) increases it will allow large amounts of fluid to flow into the tissue. Since delta V (volume ) is indirectly proportional to delta P ( pressure ), as pressure increases, the potential volume decreases. In essence, the gel becomes less viscous, increasing the free fluid space, creating the condition of Edema. While in the standing position, gravity pushes the free fluid from the upper body to the lower body which is why edema shows up in the feet. As we stated before in part XI, hydrostatic and osmotic pressure of the blood capillaries force fluid out of the blood from the arterial ends, as they join the lymphatic capillaries, which then reabsorb the fluid at the venous end, just before entering the heart. However, around 3 litres of fluid is left behind in the tissue spaces which becomes part of the interstitial fluid ( fluid outside of the cells ), that must be ‘vacuumed up’ by the lymphatic vessels, part of the lymphatic capillary system, where the fluid is termed ‘Lymph’ ( clear water ) and fed back into the bloodstream within the lymphatic one way system toward the heart. The lymphatic capillaries and the endothelial cells that form the capillary walls act like flaplike minivalves ( revolving doors ). When the the fluid pressure is higher in the interstitial fluid these valves open allowing fluid to drain into the lymphatic capillaries, but if the pressure is higher in the lymphatic vessels these valves flap shut. So an important function of the lymphatic drainage is to return the lymph to the general circulation. This accumulated fluid and proteins, filtered from the capillaries into the interstitium, prevents the interstitial hydrostatic pressure to become positive. When the interstitial pressure increases, the lymph flow increases, clearing proteins away from various body cavities including synovial cavities such as in the knees. So as mentioned before, injury or infection causing inflammation in any of the body cavities can potentially block the flow of lymph, inducing this cascade of pressure differential, causing the edema condition.
Group Capt. Lionel Mandrake: “Do I look all rancid and clotted? You look at me, Jack. Eh? Look, eh? And I drink a lot of water, you know. I’m what you might call a water man, Jack – that’s what I am. And I can swear to you, my boy, swear to you, that there’s nothing wrong with my bodily fluids. Not a thing, Jackie”
Movie quote Dr Strangelove
Check out other Articles in this series:
Nutrients in Food and their bodily purpose I (Phenols)
Nutrients in Food and their bodily purpose II (Lignans, Triterpenes, Phytosterols, Carotenoids & Fats)
Nutrients in Food and their bodily purpose III (Phenolic acids, sulphur, sulphides,sulphoxides )
Nutrients in Food and their bodily purpose IV (Glucosinolates, Sulforaphane, Indole-3-Carbinol)
Nutrients in Food and their bodily purpose V (Lipid distribution, absorbed fats, Criciferous Veg)
Nutrients in Food and their bodily purpose VI (Nutrients required for Liver Detox)
Nutrients in Food and their bodily purpose VII (Seeds & the Omega Fatty Acids)
Nutrients in Food and their bodily purpose VIII (Nutrients required for cellular energy production)
Nutrients in Food and their bodily purpose IX (Water I Properties and Body fluids)
Nutrients in Food and their bodily purpose X (Water II Cellular Hydration)
Nutrients in Food and their bodily purpose XI (Water III Fluid filtration, reabsorption, excretion)
Nutrients in Food and their bodily purpose XII (Water IV Blood pressure, Blood volume regulation)
Nutrients in Food and their bodily purpose XIV (Dental Nutrients)
Nutrients in Food and their bodily purpose XV (Nutrients involved in Methylation I)
Nutrients in Food and their bodily purpose XVI (Nutrients involved in Methylation II)
Nutrients in Food and their bodily purpose XVII (Nutrients involved in Methylation III)
Nutrients in Food and their bodily purpose XVIII (Nutrients involved in Methylation IV)
Nutrients in Food and their bodily purpose XIX (Methylation V and the Microbiota I)
Nutrients in Food and their bodily purpose XX (Methylation VI and the Microbiota II)
Nutrients in Food and their bodily purpose XXI (Superfoods: Wheatgrass)
Nutrients in Food and their bodily purpose XXII (Superfoods: Adaptogens)
Nutrients in Food and their bodily purpose XXIII (A look into our nutritional past Sir Robert McCarrison)
Nutrients in Food and their bodily purpose XXIV (Pregnancy: Nature vs Nurture vs Nutrition)
References/Acknowledgments :
- Essentials of Human Anatomy & Physiology 2000 Elaine Marieb
- Textbook of Medical Physiology 2006 Guyton & Hall
- Syndrome of inappropriate antidiuretic hormone secretion (SIADH), Compliance (Physiology), Hyponatremia, Edema Wikipedia
- Body fluid volume ScienceDirect
- Epigenetics The death of the genetic theory of disease transmission 2014 Joel Wallach
- Capillary exchange Anatomy and Physiology II ER services
- Dr Strangelove movie quotes 1964 Ranker
Author: Eric Malouin