Introduction
In this article I would like to explore Psychiatry and their use of pharmaceutical drugs such as Prozac, and the readiness to prescribe drugs for psychiatric disorders without trying to find the root cause of the disorder.
Psychiatrists behave in the same manner as conventional allopaths pushing drugs for the quick fix and symptom suppression.
Physicians support this practice by reporting that there is lack of time and the meager availability of other therapies, which i might add is possibly true given the time constraints imposed on Medical physicians in terms of face to face time with patients by the Medical system.
Antidepressant drugs are by far the most pervasive by ‘medicalising’ unhappiness.
Psychiatric care is yet another example of selling sickness and common human afflictions like Sadness, Melancholy, and Unhappiness are being converted into medical conditions which are then treated with drugs.
One of the most influential anti-depressant pharmaceuticals is Fluoxetine Hydrochloride otherwise know as ‘Prozac’ that was first marketed in 1988 by Eli Lilly which was the first SSRI (Selective Serotonin Reuptake Inhibitor). Let us analyze this a little further….
Antidepressant Drugs:
SSRI (Selective Serotonin Reuptake Inhibitor)

The development of these drugs stemmed from a theory that depression is caused by a chemical imbalance in the brain, specifically low serotonin levels known as the ‘Serotonin hypothesis’ where it was surmised that an SSRI class of drug will increase your serotonin levels and you can be happy again.
Unfortunately, biology is not that simple, as you may have gathered from the plethora of articles on this website.
You only need to research the drug Tianeptine (Trade names Stablon,Coaxil,Tatinol) which is also an antidepressant and used for the treatment of major depressive disorders as well as the treatment of asthma and Irritable Bowel syndrome (IBS).
Since it is only marketed in Europe (not in the UK,Australia or North America) it is non competitive toward Prozac.
The interesting fact about this drug is it is an SSRE (Selective Serotonin Reuptake enhancer) which means that it is an enhancer not an inhibitor (SSRI). The SSRE improves serotonin reuptake (as opposed to blocking the reuptake of serotonin as does the SSRI) by lowering the synaptic concentrations (as opposed to increasing pre-synaptic neuron density because Serotonin is not being recycled) and reducing serotonergic neurotransmission ( as opposed to having serotonin continually flowing as in SSRI’s).
The research shows that it is just as effective as Prozac with less side effects.
Therefore this flies in the face of the science that depression is caused by low serotonin levels which by now, most scientists on the planet believe that this is and was an erroneous theory.( Ref : From Serotonin to Neuroplasticity: Evolvement of Theories for Major Depressive disorder 2017 Bangshan Lit et al) .it is more of a Serotonin imbalance caused by an imbalance in the gut.
However, the Pharmaceutical industry marches on with the same failed theory to market their antidepressants. Today the field has expanded to interfere with other cranial neurotransmitters and manufactured drugs now include:
- serotonin and norepinephrine reuptake inhibitors (SNRIs)
- tricyclic antidepressants (TCAs)
- tetracyclic antidepressant
- dopamine reuptake blocker
- 5-HT1A receptor antagonist
- 5-HT2 receptor antagonists
- 5-HT3 receptor antagonist
- monoamine oxidase inhibitors (MAOIs)
- noradrenergic antagonist
I must add, that this website Healthline also suggests something more natural like St. Johns Wort or supplemental S-Adenosyl-l-Methione (SAMe).
Another tool used by the pharmaceutical industry, in this case Eli Lilly makers of Duloxetine (SNRI Antidepressant) was the use of a questionnaire that appeared on the WEBMD website, basically requiring people to perform their own diagnosis of possible depression by asking:
“I feel sad or down most of the time”
“I feel tired almost every day”
“I have trouble concentrating”
“I feel worthless or hopeless”
If you answered NO to every question and then pressed the ‘Submit‘ button the following response was:
Lower risk…..You may be at risk for major depressions
WHAT DOES THIS MEAN???..you answered NO to every question and they say you are at risk of major depression..how did they come up with that conclusion…I know..they realised that you are probably on your way to being depressed because you lied in answering the questions..that must be it…lol.
“This is really selling sickness in the sickest sense.”
The Science Behind Serotonin

To continue our discussion on serotonin I would like to lean on the great work of Michael Gershon who in the early 1980’s was attempting to ‘track down’ Serotonin distribution in the body as part of his research on the Enteric Nervous System, which he termed our ‘Second brain’ (the gut).
As he points out, even in 1981, scientists accepted that 99% of Serotonin is manufactured in the gut and 1% is produced by the brain (simply a minor supplement).
The lion’s share of Serotonin is actually stored in the bowel so it is conceivable that not only is Serotonin a neurotransmitter for the brain but it is also a neurotransmitter for the enteric nervous system.
This is evident since anybody taking SSRI’s experience nausea and vomiting which then leads to diarrhea and then constipation because the drug is interfering with this crucial neurotransmitter needed for natural bowel movement.
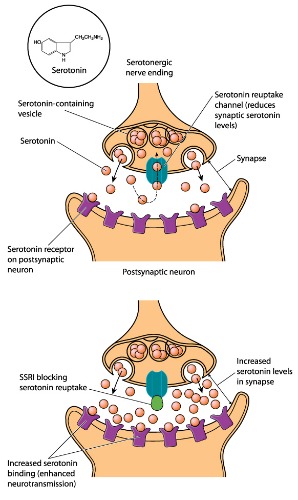
What occurs naturally is that Serotonin in the nervous system and the enteric nervous system is turned off by the reuptake of serotonin by the Serotonin-containing nerves that release it, and then recycled.
It is the Serotonin transporter that is key to the Serotonin reuptake, recycling and inactivation.
The SSRI drug in effect, inhibits the Serotonin transport, and in turn inhibits reuptake,recycling and inactivation.
The initial effect of this inhibition causes neurotransmitter potentiation (the signal between synapse junctions strengthen) and by taking the drug for a period of time causes Long term potentiation or synaptic elasticity:
Synaptic junctions are not hard wired together but communicate between each other using neurotransmitters and as the neurotransmitter becomes stronger more ions like calcium etc are allowed to flow across the synapse, increasing potential across the post synaptic neuron membrane.
This is how learning and memory is achieved, using the same mechanism where post synaptic neuron strength depends upon potentiation (signal strength of the neurotransmitter coming from the stimulated serotonin-containing nerve cell).
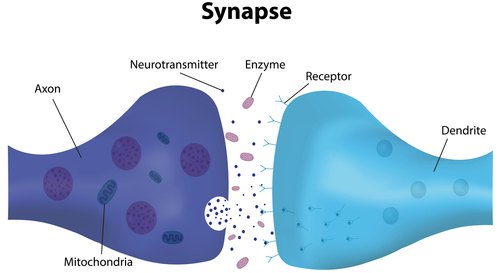
By blocking the normal Serotonin reuptake from the synapse, Serotonin stays in the synapse longer and the body’s natural feedback mechanism causes the pre-synaptic neuron to down regulate releasing less Serotonin while the post-synaptic neuron (the receiver) down regulate its receptors.
The drug is acting as a Serotonin Accelerator while the body’s applying the brake.
Overtime, this interference of the Serotonin process causes some Serotonin receptors to desensitize and fail to respond anymore, while others become less sensitive to stimulation by Serotonin.
Other nerve cells treated with this drug will produce less Serotonin.
Because Serotonin is used in the enteric nerve system, the bowel writhes and churns, and then freezes up causing bowel disturbance.
Some anti-depressant takers report that they feel relief from their depression..HOW..only to end up with all these gastrointestinal problems which is enough to become depressed again.
At one stage the drug manufacturers were trying to separate the side effects of the drug in the gut and the antidepressant direct effects..GOOD LUCK.
Serotonin the End Game
What the drug companies fail to appreciate is that Serotonin or 5-hydroxytryptamine (5-HT) is predominantly produced by Enterochromaffin (EC) cells situated in the gastrointestinal tract, but it is our bacterial neighbours, specifically 20 species (approx) of Spore Forming Bacteria that elevate the production of serotonin (without these bacteria the EC cells would make considerably less, approx 60% less).
This Bacterial/Host collaboration is not fully understood, only that the metabolites (products of the microbe,s metabolism) are regulated by these spore forming bacteria that elevate Serotonin levels in the EC cells by a stimulation affect.
We also know that other bacteria produce Serotonin alone.
Therefore, for these drug companies to believe that by inhibiting the Serotonin transport is an answer to treating depression efficiently is folly.
This is evidenced by the mechanism of action provided by Tianeptine which functions in an opposite way to the SSRI.
We have already stated in the articles on the Microbiome that disorders that affect cognitive and mood disorders such as Autism, Dyslexia, Dyspraxia, ADD, ADHD, Schizophrenia and Depression are all digestive disorders driven by a dysbiotic gut, allowing non beneficial flora overgrowth to release their toxins, which eventually cross the blood brain barrier, causing a chemical imbalance in the brain.
In my opinion it makes sense that depression can only be treated naturally without dangerously altering chemical pathways in the brain.
Furthermore, depressive individuals whose gut is in chaos are more likely to produce an imbalance of Serotonin affecting their gut, bowel function, and their cognitive function together.
As I said before, Serotonin levels in the brain and the manipulation of the serotonin transport is doing something, I don’t know what, except wrecking the neuron cell receptors and eventually depriving them of normal function when the problem in the gut is solved.
The Antidepressant Chronicles
Corruption

So when Prozac was introduced in 1988, the German regulator concluded that Prozac was totally unsuitable for the treatment of depression and the FDA noted serious flaws in the trials, but the company Eli Lilly depended on the success of this drug in order for the company to survive.
The General Manager for Eli Lilly Sweden at that time John Virapen (you can see his YouTube videos or read his book ‘Side Effects: Death. Confessions of a Pharma insider) who knew his future depended on the success of Prozac, so according to Peter Gotzsche’s in his book ‘Deadly medicines and Organized crime’ he relates the story of how Virapen organised seeding trials and invited doctors to the Caribbean for a week to include ‘diving, surfing, sailing, girls and hot nights.
He then went on to bribe the independent expert who was supposed to examine the data on the drug and recommend approval or not.
As a result, according to Gotzche, it was a $20,000 bribe, and the expert then requested that Lilly provide research money.
Furthermore one of Viraprens associates met with the expert to improve the drug registration by burying the evidence that during the trials of the drug, 5 of the test subjects had hallucinations and tried to commit suicide, and 4 of them were successful in ending their lives.
Virapen and 2 other associates were dismissed from the company after the drug was approved..expendable assets.
Litigation

The New York times reported in 1990 that 6 lawsuits had been filed seeking a total of $300 million in punitive and compensatory damages accusing the drug company, makers of Prozac of improper testing of the drug and not warning doctors that this antidepressant drug may in some cases ignite aggressive, violent or suicidal behaviour.
The lawyers involved, relied on a report published by Dr Martin Teicher and his colleagues of Harvard Medical school describing 6 patients who began to have suicidal thoughts after being prescribed Prozac.
In 2006 the European Medicines Agency (EMA) stated that :
“The Agency’s scientific committee, the Committee for Medicinal Products for Human Use(CHMP), concluded at its 19-22 April 2005 meeting that suicide-related behaviour (suicide attempt and suicidal thoughts), and hostility (predominantly aggression, oppositional behaviour and anger) were more frequently observed in clinical trials among children and adolescents treated with these antidepressants compared to those treated with a placebo pill (that contains no active medicine).”
Addiction

The other problem with antidepressant drugs for some, can create a dependency or addiction, after all they are trying to treat depression and if it works either by the combination of the medicine and the biology, and/or the belief of the individual, it is obvious that the patient will want more, since they feel better and they want to maintain that state of mind.
I don’t specifically believe it is a particular drug, maybe some are more prone toward habit forming than others, but its no different than taking heroin or cocaine.
Most people are under some illusion that since these are legally prescribed approved drugs they are not potentially addictive, but in some individuals depending on their circumstances withdrawal symptoms have been reported to have occurred.
GSK (Glaxo Smith Kline) in 1992 claimed that their antidepressant Paxil was not addictive, despite the original licence application stating that 30% of patients during the trials displayed withdrawal symptoms.
This is what is written on the UK Medicines & Healthcare products Regulatory Agency (MHRA) website concerning SSRI/SNRI’s use and safety :
“All SSRIs and SNRIs may be associated with withdrawal reactions on stopping or reducing treatment. Symptoms of withdrawal such as anxiety, agitation and insomnia have been reported after a dose decrease or stopping treatment with SSRIs and SNRIs.
Previous safety considerations on SSRIs led to updated warnings for all SSRIs on the potential risk of withdrawal reactions after stopping treatment.
Further assessment of available evidence by an expert group on the safety of SSRIs led to the following conclusions on withdrawal:
-
all SSRIs and SNRIs may be associated with withdrawal reactions on stopping or reducing treatment
-
paroxetine and venlafaxine seem to be associated with a greater frequency of withdrawal reactions than other SSRIs – the most commonly experienced withdrawal reactions are:
- dizziness
- numbness and tingling
- gastrointestinal disturbances (particularly nausea and vomiting)
- headache
- sweating
- anxiety
- sleep disturbances
-
awareness of the risk of withdrawal reactions associated with SSRIs and SNRIs needs to be increased among both prescribers and patients
-
withdrawal reactions are less severe when the dose is gradually decreased or ‘tapered off’ over several weeks’
Suicidal Thoughts
In terms of suicidal thoughts again the MHRA state:
‘There is a risk of suicidal behaviour with the use of any SSRI or SNRI, particularly when used by children, adolescents or young adults. SSRIs and SNRIs are effective medicines, and the balance of risks and benefits in adults of all medicines in these drug classes remains positive in their licensed indications.
However, some cases of suicidal thoughts have been reported with SSRI and SNRI use. MHRA and Commission on Human Medicines (CHM), have investigated and monitored this safety issue since these products were first licensed.
In May 2003, an SSRI expert working group was established to consider the safety of SSRIs, including the issue of suicidal risk.
The group reviewed all available data and concluded the following that:
-
generally in depressed patients the risk of suicide is greatest around the time of their presentation to medical services, however the risk of suicide may increase in the early stages of treatment for depressive illness
-
a modest increase in the risk of suicidal thoughts and self-harm for SSRIs compared with placebo cannot be ruled out
-
there is insufficient evidence of any marked difference in suicidal risk between the different SSRIs, or between SSRIs and other antidepressants.’
Depression

In the 1990’s Professor Rif El-Mallakh of the mood disorders research program department of Psychiatry and Behavioral sciences, University of Louisville School of Medicine, published a paper providing an overview of ’emerging evidence that, in some individual’s constant use of anti-depressants may cause pro-depressant effects.
What he was saying was that persistent use of antidepressants created a treatment resistant depression which applied to some 10-15% of antidepressant takers in the 1990’s which exploded to 40% in 2006.
Furthermore, in 2011 he states that 80% of patients suffer symptom recurrence due to this treatment resistance and the continual prescriptions may lead to permanent chronic depression.
The pathology explained above, concerning the effect of SSRI interference of Serotonin acceleration and the body’s adaptation of trying to apply the break probably leads to ‘permanent down-regulation of correction’.
In the same way, this permanent down-regulation of correction occurs when hormones are injected into the body over time, instead of fixing the gland, the body shuts down glandular function, similarly blocking cholesterol production with drugs causes the body to shut down fructose metabolism by the liver and the muscles take over the function to compensate causing muscle wreckage over time (just check the side effects of statins..muscle pain and weakness).
Professor El-Mallakh remarks that people who take anti-depressants for anxiety and/or panic disorder who are not depressed initially, may become depressed even after the drug is withdrawn.
This not only Selling Sickness, it is Selling Depression.
A condition known as ‘Oppositional tolerance’, a condition that psychiatrist Giovanni Fava (editor of Psychotherapy & Psychosomatics) wrote about in 1994, which also occurs with long term use of anti-psychotic drugs (e.g Neuroleptic medicine used to treat psychosis like delusions,hallucinations, paranoia, schizophrenia, bipolar disorder, obsessive compulsive disorder, Post traumatic stress disorder).
Medicines like Olanzapine( Brand name Zyprexa), used to treat schizophrenia and bipolar disorder which is a Dopamine Antagonist and chemically similar to Benzodiazepine.
The symptoms of Oppositional tolerance from long term use of antipsychotic drugs can cause Tardive dyskinesia (TD), a condition that results in involuntary repetitive body movements including grimacing, sticking the tongue out, lip smacking, rapid jerking movements or slow writhing movements.
This indicates that the Basal Ganglia, situated at the base of the Forebrain connected to the Cerebral Cortex and the Thalamus that is responsible for voluntary motor control, procedural learning, eye movement, cognitive and emotional functions, has been damaged by these drugs.
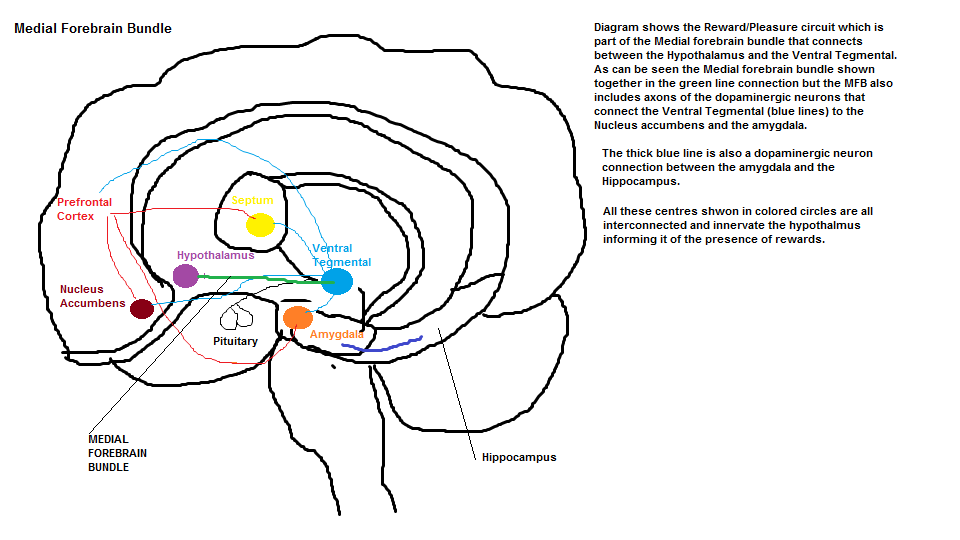
Again, a plausible physiological explanation has been put forward, since Dopamine (a neurotransmitter that regulates/controls our reward/pleasure circuit located along the Medial Forebrain Bundle (MFB) depicted below in the diagram below) is being interfered with.
Dopamine receptors (D2 receptors) are blocked, and the body’s compensatory response is to increase the density of the D2 receptors causing ‘supersensitivity’; thus leading to constant firing of the neurons controlling motor movement, and in some cases the damage becomes permanent even after the drug is withdrawn.
In essence the longer the individual is on the anti-depressant, the more likely they are to relapse.
Paul Andrews and his colleagues at Virginia Commonwealth University confirmed these findings and likening it to pulling a spring from its equilibrium position.
When this happens the spring would oppose the movement, and the greater displacement from its equilibrium position, the greater the oppositional force.
A French study confirmed this as well using 35,000 patients.
The STAR*D (Sequenced Treatment Alternatives to Relieve Depression) funded by the National Institute of Medical Health (NIMH) conducted in 2006 discovered that 108 patients out of 4041 left the trial and stayed well during the year long follow up to the study.
The other 3,933 relapsed or dropped out.
In 2010 the MN Community Measure organization from Minnesota who gathers data on health outcomes in Minnesota reported that only 5.8% of 23,887 patients treated for depression were in remission at the end of 6 months, and 4.5% in remission at the end of 12 months, which means that 95% of the depression patients in Minnesota are still chronically depressed.
Conclusion
I have to conclude that anti-depressants can and have helped people I am sure, but if you take a drug to interfere with natural cranial chemistry which is already compromised, you are playing ‘Russian roulette’ and you cannot anticipate the outcome individually.
Unfortunately, because of past events, you cannot believe the pharmaceutical companies or the physicians in terms of the mechanism of drug actions, specifically the multitude of side effects which I must say are quite well documented on various websites so you can do your own research.
Drug companies are not going to put their products in a bad light because that would be foolish..how many times have you been to a restaurant and heard people ask “ How are the enchiladas ?”..the waiter is not going to say they’re crap..because he’s ‘biting off the hands that feed him’.
Even in 1880’s the UK government did not think that opium use in India caused any adverse reactions, in the same vain as doctors in the 1960’s believed that Benzodiazepines (Valium) were harmless little pick-me-ups.
The UK regulator at the same time, reported that only 28 people taking Benzodiazepines between 1960-1977 became dependent on the drug but we can only guess that this number was probably in the thousands.
Given the terrible statistics from the previous paragraph on the number of chronically depressed people in one state, and the fact that long term use of anti-depressants can lead to ‘Oppositional tolerance’ and/or Tardive dyskinesia (TD), think twice before you allow your children to be prescribed with these ‘medicines’ or even yourself.
I personally have not been depressed so I can’t say I speak from experience but I was around someone who was chronically depressed and I can say it is a miserable, character shape shifting condition making that person vulnerable to anyone telling them that these anti-depressants will help them and they would not even care about the possible long term affects, but just to seek some relief.

[Tony urges Dr. Melfi to get out of town for a while]
Dr. Jennifer Melfi: I have patients who are suicidal!
Tony Soprano: Well they’re not gonna feel any better about their life if you get clipped.
Dr. Jennifer Melfi: Isn’t it interesting how this memory loss cropped up right after you failed to be killed in the carjacking? You think it was a carjacking?
Tony Soprano: Of course not, but I got an idea who was behind it. Enough said. You don’t want to go there.
Dr. Jennifer Melfi: Maybe you don’t want to go there.
Tony Soprano: What are you talking about?
Dr. Jennifer Melfi: Well, let’s track it. Right around the time of the shooting, you were having hallucinations of that Isabella figure. The protective, loving mother. Your subconscious was shouting something at you. On the day before the shooting, you said to me that she kept going on yet again about news stories of mothers throwing their babies out of windows.
Tony Soprano: Why don’t we put our cards on the table here. What do you think, my mother tried to have me whacked ‘cuz I put her in a nursing home?
Dr. Jennifer Melfi: It’s been a long odyssey with your mother, hasn’t it?
Tony Soprano: Oh, these last 500 years just seemed to race by.
The Sopranos: I Dream of Jeannie Cusamano (#1.13)” (1999) quote
Check out the Previous Article in this series:
https://www.extremehealthacademy.com/selling-sickness-part-1-conventional-medicine-is-a-business/
https://www.extremehealthacademy.com/selling-sickness-part-2-profits-before-health/
https://www.extremehealthacademy.com/selling-sickness-part-3-baffling-the-masses/
https://www.extremehealthacademy.com/selling-sickness-part-4-prostaglandin-drugs/
References/Acknowledgments:
- Bad pharma how drug companies mislead doctors and harm patients Book 2013 Ben Goldacre
- What medications help to treat depression Healthline 2017 Kristeen Cherney
- Microbes help produce serotonin in the gut CALTCH 2015
- Deadly medicines and organised crime book 2013 Peter Gotzche
- Tardive dyskinesia, Anti-psychotic Wikipedia
- Eli Lilly facing million dollar lawsuit on its antidepressant drug Prozac HEALTH Natalie Angier aug 1990
- Serotonin specific reuptake inhibitors & Serotonin noradrenaline reuptake inhibitors EMA
- SSRI’s, SNRI’s use & safety Medicine & Healthcare products Regulatory Agency (MHRA) Dec 2014
- New Antidepressant induced chronic depression has a name : Tardive Dysphoria Robert Whitaker Jun 2011 Psychology today
- The role of the Basal Ganglia in movement
- The Brain from top to bottom: The reward circuitmcgill.ca
- Q&A about the NIMH Sequenced Treatment Alternatives to Relieve Depression (STAR*D) Study All medication levels National Institute of Mental Health (NIMH) Nov 2006
Author: Eric Malouin