Introduction
In this article we will list the current vaccines and discuss societies vaccine reference the Infant Mortality Rate (IMR) and an in depth look at the DpaT (Diphtheria-Pertussis-Tetanus) vaccine.
Vaccines

Vaccines existed in the fifties in 2 varieties where Salk’s vaccine was a ‘Killed’ virus and Sabin’s was an attenuated ‘Live’ vaccine. Today there are 3 other types Toxoid, Subunit and conjugate varieties. The following list shows the 5 types of vaccine used today:
Live, attenuated vaccine list:
- Vaccinia (smallpox)
- Measles, mumps, rubella (MMR combined vaccine)
- Varicella (chickenpox)
- Influenza (nasal spray)
- Rotavirus
- Zoster (shingles)
- Yellow fever
Inactivated/killed vaccine list:
- Polio (IPV)
- Hepatitis A
- Rabies
Toxoid (inactivated toxin) vaccine list:
These vaccines are made from inactivated toxic metabolites of certain bacteria and attached to adjuvants like aluminium or calcium salts to elicit a strong enough immunological response, but will require several doses.
- Diphtheria, tetanus (part of DTaP combined immunization)
Subunit/conjugate vaccine list:
(Subunit vaccines use the disease causing part of the virus (the protein or Antigens 1-20) are either extracted directly from the virus or grown in the lab using Virus DNA/ Protein-polysaccharide conjugation which is a process whereby a poor antigen (polysaccharide) is attached to a strong antigen to supposedly elicit a stronger immunological response. Conjugate vaccines were developed to increase longer term immunity where T cells are activated by the vaccine which in turn secrete cytokines to elicit a long term memory response.
- Hepatitis B
- Influenza (injection)
- Haemophilus influenzae type b (Hib)
- Pertussis (part of DTaP combined immunization)
- Pneumococcal
- Meningococcal
- Human papillomavirus (HPV)
Vaccine Types: Pros/Cons

Live, attenuated
The advantage with this type of vaccine is that it is as close to natural infection/immunity with a difference, because they have been weakened that are unable to reproduce the thousands of times required to infect the host with the disease, but can only reproduce fewer than twenty times. It only requires one to two doses to acquire lifelong immunity. Having said that there still exists a risk that the virus can take hold especially if the host has a compromised immune system so the host must be examined to establish a healthy immune system. This is not the case however, with a disease causing bacteria since Viruses exist with few genes whereas bacteria exists with thousands of genes, although science is attempting to isolate key genes in bacteria that can be removed thus weakening (attenuating) the bacteria. Transportation of live viruses is problematic since they are sensitive to light and heat so they must be refrigerated.
Inactivated/killed
This type of vaccine is safer and more stable than its ‘Live’ counterpart since the virus is dead and cannot be resurrected, in addition no refrigeration is necessary. However, its activated response to the host immune system is much weaker so it requires an adjuvant to stimulate the immune system to produce anti-bodies, several doses are required to elicit a response, and booster shots are also required to maintain immunity. The current polio vaccine is of this type (the original Salk vaccine).
Toxoid (inactivated toxin)
The advantage is that the vaccine cannot cause the disease and is stable, but it requires multiple dosing and it needs an adjuvant.
Subunit/conjugate
The advantage in using Subunits is that it can be used in people with weak immune systems, provide lifetime immunity and adverse reaction is low, The disadvantage is that several doses must be given to provide long time immunity.
Infant Mortality Rate (IMR)

Before we get into the specifics of the various vaccines, the main reason for vaccines is to sustain a healthy infant mortality rate..right?. There are various factors that drive IMR. The World health organisation claims that 7 out of childhood death in developing countries is Pneumonia, diarrhea, measles,malaria and malnutrition where malnutrition affects the immune system and drives the rest of the causes because the children are defenceless with a compromised immune system, and thus any nutritional deficiency will diminish resistance to disease….this statement was in a scientific article in PubMed ??…I think the message is finally getting through. Singapore,Sweden and Japan have an IMR rate below 2.8/1000 births which is < half the rate of the US yet the US spends more per capita on healthcare than any other country..eh let’s rephrase that a little..the US spends more money with the Pharmaceutical industry than any other country..that does not necessarily equate to health care..it just means big Pharma have a bigger vacuum cleaner than anybody else. The CDC stated that:
“The relative position of the United States in comparison to countries with the lowest infant mortality rates appears to be worsening.”
IMR is also affected by risk associated with premature births (an increase of 20% in the US between 1990-2006) and preterm births. There is also a distinct possibility that immunization and vaccine requirements also play apart. In 2009 5 of the 34 nations with the best IMR’s require only 12 vaccine doses for infants < a year old compared to 26 doses in the US. Here are several IMR examples:
- Singapore = 2.31
- Czech republic = 3.79
- Spain = 4.21
- UK = 4.85
- US = 6.22
It is a fact that Gambia who requires its infants to receive 22 vaccine doses with a 95-98% national vaccine coverage yet its IMR = 68.8, and Mongolia almost mirrors Gambia and their IMR is 39.9. We know that these nations are not a developed as the US, but what does that mean, the US has better infrastructure, better communications, better health (????), more drugs, more fast food, more processed food..well maybe that’s the problem. More vaccines, more doses given to infants that are born from most mothers that are consuming this stuff, so the mother’s immune system and that of her newborn is potentially compromised. The fact that sanitation and clean water (???…does that mean more fluoride) and access to health (another problem) is better in the US than developing countries has very little relevance in terms of IMR it seems. So where does the US value of 6.22 derived from ?. In 2009 there were approximately 4.5 million live births and 28,000 infant deaths which is equal to 6.22/1000.
SIDS/SUIDS
Furthermore, Sudden Infant Death syndrome (SIDS) became a statistic in 1973 in the National center for health statistics and by 1989 became the leading cause of post-neonatal mortality ( 28 days-1 year old). Autopsies revealed that in most cases congestion and edema of the lungs and inflamed respiratory systems were the cause. The American Academy of pediatrics began suggesting to parents that their infants should be placed supine (face upward) as opposed to prone (face downward) during sleep in an effort to reduce SIDS which it did by an average of 8.6% between 1992-2001. Then SUIDS (sudden unexpected infant death -due to asphyxia) became a factor and increasing.
SIDS/SUIDS and VACCINES
Coulter and Fisher in 1985 reported 6 children that were statistically categorized under the SIDs umbrella, five of which died within 48 hours of receiving the DPT shot. Torch in 1986 summarized case reports where 150 died post DPT vaccination (reported by 37 different authors in 12 countries where 50% of mortality occurred within 24 hours, 75% within 72 hours and 90% within 1 week following DPT administration. It is reported that in the US approximately 55 cases of SIDS/year are to be expected within 24 hours of receipt of the DPT vaccine as published by Stetler et al in 1985. Torch also reported in 1982 70 of 200 (35%) infant mortality cases that were clustered cases of SIDS within the first 2-3 weeks of receiving the DPT vaccine. Baraff and colleagues in 1983 interviewed 145 of 382 parents (38%) who were SID infantile victims during a 20 month period where 53 cases had received the DPT vaccine prior to death, 11% within 1 day of death, 32% within 1 week of death and 51% within 4 weeks of death.
The CDC through their VAERS (Vaccine adverse effect reporting system) for the period 1978-1990 80 million doses of DPT were administered and 350 case reports were received , 332 (94.9%) occurred in infants who had received at least one DPT shot. Analyzing the data 350 cases from 80 million DPT shots in 12 years may not seem a lot, but most people during that time were unaware of VAERS so the number is probably much higher. There are many more SIDs/Vaccine associations such as 222 deaths in Norway reported as SID cases from 1975-1982 (Solberg 1985), and of these cases 53 deaths occurred within 4 weeks of receiving the DPT shot. Finally the largest study is the NICHD SIDs Cooperative epidemiological study ( Hoffman et al 1987) where all SID cases were identified in 6 US states where there were 350,000 live births over a 15 month period in 1978/79. There were 716 SID cases reported, 40% of which had received a DPT shot. As the voice of the supreme court in the US stated:
“Vaccines are Unavoidably Unsafe.”
Torch from his study concluded that:
“That DPT may be a generally unrecognized major cause of sudden infant and early childhood death, and that the risks of immunization may outweigh its potential benefits. A need for reevaluation and possible modification of current vaccination procedures is indicated by this study”

Vaccine Ingredients
So let us examine the ingredient of the DPT or DtaP as it is also know which stands for Diphtheria-Pertussis-Tetanus vaccine. There are 2 versions of it Daptacel and Infanrix:
| VACCINE | INGREDIENTS | COMMENTS |
| DtaP (Daptacel)
Manufacturer : Sanofi-Pasteur (US: 3 doses – 2/4/6 first months of life) (UK: 5 in 1 incl polio/Hib 2/3/4 first months of life) (Australia 2/4/6 first months of life) |
Aluminium Phosphate
Formaldehyde Glutaraldehyde 2-Phenoxyethanol Stainer-Scholte medium Casamino acids Dimethyl-beta-cycolextrin Mueller’s growth medium Ammonium sulphate Modified-Miller casamino acid medium w/o beef heart infusion |
Adjuvant to stimulate IS
To ensure virus is inactivated Disinfectant Preservative Growth medium for Bordetella pertussis toxin Stabilizer Muscle extracts to produce tetanus toxin Strain of Clostridium tetani used as culture medium |
| DtaP (Infanrix)
Manufacturer : GSK |
Fenton medium with Bovine extraction
Modified Latham medium derived from Bovine casein Formaldehyde Modified Stainer-Scholte liquid medium Glutarldehyde Aluminium hydroxide Sodium chloride Polysorbate 80 |
Ingredient from beef cattle
Mixture of various vitamins, iron,NaCl,Mag sulfate,cystine Adjuvant Surfactant and emulsifier |
More information on these vaccines including possible adverse reaction can be found on the following website:
http://www.nvic.org/Vaccines-and-Diseases/Whooping-Cough.aspx#vaccine

DTaP Effectiveness
Please bear in mind that the CDC Epidemiology and Prevention, The Pink Book 6th edition, Chapter 6 Pertussis pg 80 states:
“There is no distinct syndrome from vaccine administration, and therefore many temporally associated adverse events probably represent background illness rather than illness caused by the vaccine….”
“The DtaP may stimulate or precipitate inevitable symptoms of underlying CNS disorder such as seizures, infantile spasms, epilepsy or SIDS.”
“By chance alone, some of these cases will seem to be temporally related to DtaP.”
Diphtheria
In a recent article abstract on the NCBI website, it was reported that a cohort study of infants born at Kaiser Permanente Northern California from 2010-2015 the estimated effectiveness of vaccine protection for newborns from pertussis (Whooping cough) was high. Among 148,981 newborns the effectiveness of TdaP was 91.4% effective during the first 2 months of life, and 69% during the entire first year of life. According to a WHO report cases of diphtheria globally were hitting the 100,000 mark but steadily declined to 5000 which are currently reported annually. There was a severe outbreak within the Russian federation in the 1990’s which left in its wake 157,000 cases and 5,000 deaths (64-76% among those aged 15 years or older, and according to the report was caused by poor vaccine coverage. Failure to administer the DtaP booster shot at school entry (age 6) to 9 ‘fueled the fire’ as well. The most severe cases occurred in the 40-49 age bracket, who were infants when the DTP was introduced to the then Soviet Union and many were not vaccinated neither were not exposed to the disease because of its decline. Having said that case did occur in vaccinated individuals. The WHO also stated that serologic (anti body measurement in serum ) and case control studies confirmed high vaccine effectiveness proving that failure to vaccinate was the problem rather than vaccine failure.
Pertussis
During the pre-vaccination periods in the US such as in 1934 there were 265,269 cases, in 1939 103,188 cases, and in 1941 222,202 (as you would expect since a lot of people were moving around fighting. By 1948 this number had dropped to 74,715 and by 1960 there were 14,809, It was 1948 when the DTP vaccine was introduced but the numbers of cases had already declined significantly. However, in 1950 the number shot up to 120,718 (why ??). By 1980 the number dwindled to 1,730 although the numbers rose a little to an average of 4000 through to 1993 and began rising again until by 2004 when the DTP vaccine was upgraded the number of cases were 25,827. In 2005 (25,616), 2010 (27,550), 2012 (48,277), and 2015 (20,762). To me unless I am mistaken the number of cases began rising from 1980 in the US despite the vaccine.
What most people are not aware of is that this vaccine is/was made in 2 flavors, ‘Whole cell pertussis’ and ‘Acellular pertussis’, where the former was first manufactured in 1933 and used exclusively up until 2001 when it was replaced with the latter. The whole cell variety used a live toxin (not inactivated) released by the virus and then injected directly into the patient. The first Acellular variety was manufactured in 1937 which was inactivated with Formaldehyde and made it a toxoid thus ‘hiding’ this less toxic, safer inactivated vaccine for 64 years later when they could have introduced it much earlier. After much discussion since 1978 in 1990 the CDC concluded that the live (whole cell) variety was causing acute encephalopathy up to 7 days after vaccination, and in 1993 categorically stated that it cause permanent brain damage. Since the Whole cell variety is cheaper to produce it is still used in developing countries (I see the inhabitants of Africa, India are more expendable than western inhabitants). As many as 1 in 60,000 over this period of 64 years may have suffered permanent brain damage, language difficulties, dyslexia or even autism. Furthermore a neonatal conference in 2004 concerning newborns discussed the idea of possibly resurrecting the Whole cell vaccine for newborns because antibody production is much higher in newborns than the Acellular version (don’t you just love it..to hell with risk let’s shoot these babies with the more potent form of this poison).
Tetanus
In 2015 there were 56,743 deaths due to tetanus, a condition that primarily erupts from dirty uncleaned wounds, approximately 45% occurred in South Asia and 44% in Sub Saharan Africa. The number of cases in the western world are fairly low. For example during the 1920s and 30s in Canada there were 26-55 deaths and between 2000-2013 there were a total of 42 cases reported ( 3 cases/year). Tetanus deaths have declined by 99% in the US since 1947. Between 2001-2008 a total of 233 cases were reported from 45 states, 197 of which resulted in death, while an average number of reported cases is approximately 29/year.
The Current DTaP Vaccine
The current vaccine, vaccinates against Pertussis or whooping cough but there is another viral strain floating around called Parapetussis which the current vaccine does not protect against, but despite the vaccine, people can still be infected. Having said that, this condition is not to be trifled with, since it is a respiratory condition where the virus causes a massive production of mucous within the lung which is coughed up during difficult breathing periods and can last for up to 8 weeks. Diphtheria causes the production of a membrane in the throat severely restricting the airways and in it worst form the patient can asphyxiate and die unless an immediate tracheotomy is performed to allow the patient to breathe. Finally the tetanus toxin can interfere with the neuromuscular junction between nerves and the muscle fibres by chemically amplifying the relation/contraction spasmodic state.
Barbara Loe Fisher

One of the great anti-vaccine crusaders is Barbara Loe Fisher. President of the National Vaccine Information Center (NVIC), a non-profit charity she co foundered with parents of DPT vaccine injured children in 1982. She has dedicated her time for the past 3 decades striving for vaccine safety reforms and informed consent protection in the Public health system. She is not a Doctor but has authored several books including ‘DPT:A shot in the dark’. You can research her further on her website NVIC. Her passion know no bounds when speaks of the outrageous injustices that have become synonymous with vaccine safety and mandatory vaccines and the obvious damage that is being unleashed with the sheer quantity of vaccines being pushed into infants not yet a year old. Her anger was initially fueled when her two and a half year old son in 1980 began convulsing and later developed learning disabilities with brain inflammation after his 4th DPT vaccine leading to a 12 year period where her son had to attend special need classes. Here are snippets from one of her great speeches:
We are advocating for the right to know the truth about the safety of the food we eat, the water we drink, the drugs doctors prescribe and the vaccines Americans are forced to get to attend school, and receive medical care, and hold a job.
We want government officials to explain to us why our country, which spends the most on health care and has one of the highest child vaccination rates in the world, is crippled by a chronic disease and disability epidemic that costs more than two trillion dollars a year, and has created the sickest child and young adult population in America’s history:
- 1 child in 6 learning disabled
- 1 in 9 with asthma
- 1 in 10 diagnosed with a mental disorder
- 1 in 13 severely allergic to food
- 1 in 20 epileptic
- 1 in 50 developing autism
- 1 in 400 with diabetes
We will not be silent as the biological integrity of another generation of children is destroyed in this bitter harvest that can only continue if we allow it to continue.
My son was part of the tidal wave of learning disabled children emerging in the 1980’s, growing larger in the 1990’s, and exploding in the first decade of the 21st century at precisely the same time that the federal child vaccine schedule tripled from 23 doses of seven vaccines in 1980 to 70 doses of 16 vaccines during the next 30 years?.
The U.S. Centers for Disease Control (CDC) now directs doctors to give pregnant women vaccines that were never licensed for use during pregnancy. Then, on the first day of birth and continuing throughout childhood, doctors are told to give children six dozen doses of vaccines that contain genetically engineered viruses and bacteria, plus ingredients like mercury, aluminum, formaldehyde, phenoxyethanol, gluteraldehyde, proteins, synthetic particles, antibiotics, and human, animal and insect DNA and RNA.
Where is the good science that demonstrates children are healthier when repeatedly given vaccines that artificially hyper-stimulate inflammatory immune responses 50 times before age six?
Just how sick do highly vaccinated children in America have to get before government health officials re-evaluate the assumption that more and more vaccination equals better health?
Why was the 21st Century Cures Act created by Congress and signed into law last year so FDA licensing and informed consent standards could be lowered even further? Now the skids have been greased for the pharmaceutical industry – the biggest lobby on Capitol Hill – to experiment on people without their consent, and to fast track drugs and vaccines to market even more quickly – without proving they are safe and effective first.
And why did Congress create a federal vaccine injury system administrative alternative to a lawsuit in the National Childhood Vaccine Injury Act of 1986 – but take no action when the Departments of Health and Justice systematically gutted that law and turned it into a cruel joke? Today, the majority of vaccine injured children are denied compensation so government officials do not have to admit just how many children are being brain damaged and dying after vaccination in America.
The $3.6 billion dollars in federal vaccine injury compensation that has been awarded to more than 5,000 vaccine victims since 1988 doesn’t begin to pay for the damage done, not when two out of three claims are denied, and not when drug companies have no incentive to make vaccines less harmful because all Americans are legally required to purchase and use their liability free vaccine products.
While we are all born equal, with equal rights under the law, we are not born all the same. Each one of us is born with different genes and a unique microbiome influenced by epigenetics that affects how we respond to the environments we live in. We do not all respond the same way to infectious diseases or to pharmaceutical products like vaccines and doctors cannot predict which of us will be harmed.
This means that vaccine risks are not being borne equally by everyone in society, and forced vaccination is a de facto selection of the vaccine vulnerable for sacrifice.
Why should the lives of those vulnerable to vaccine complications be valued any less than those vulnerable to complications of infections?
It was not always this way in America. I grew up in the 1950’s and 60’s and remember when every child got measles, mumps and chickenpox before age 10, but there were no special education classrooms in public schools to house legions of learning disabled, autistic and emotionally disturbed children. I remember when it was the rare child who could not learn and half of the students were not carrying Epi-pens and asthma inhalers in their pockets, and there was no need to store student supplies of Ritalin and Prozac in the school nurse’s office. I remember when we ate peanut butter and jelly sandwiches for lunch without being afraid it would kill one of our classmates.
The reaction by vaccine developers and others promoting “no exceptions” forced vaccination laws is to label parents disagreeing with them as “selfish” and to suggest they are “child abusers.” Or to insist, like pediatrician Paul Offit, that vaccine injuries and deaths are a myth and that children can safely receive 10,000 vaccines at once. Or, like pediatrician Peter Hotez to call on the U.S. government and the G20 to wage a war on American parents defending exemptions in vaccine laws.
Decisions..Decisions..

In terms of ingesting any drugs including vaccines,and I know its difficult or impossible unless you are aware of the facts, is to perform a risk benefit analysis. If the risks far outweigh the benefits it would be sensible to avoid the risk. If the situation was reversed it would be prudent to go ahead since the benefits far outweigh the risks. This equation however is highly variable on both sides and in some respects it’s the ‘roll of a dice’ so to speak. In the last 200 years or so the various communicable diseases Diphtheria, whooping cough, measles, smallpox etc did not erupt due the deficiency of a vaccine but more life lifestyle, effective sanitation, hygiene. Close quarter living etc provided the breeding ground for these diseases. Most, if not all of known epidemics caused by disease declined naturally due to improved living conditions etc. This is borne out from the graphs below which clearly display this point of view:
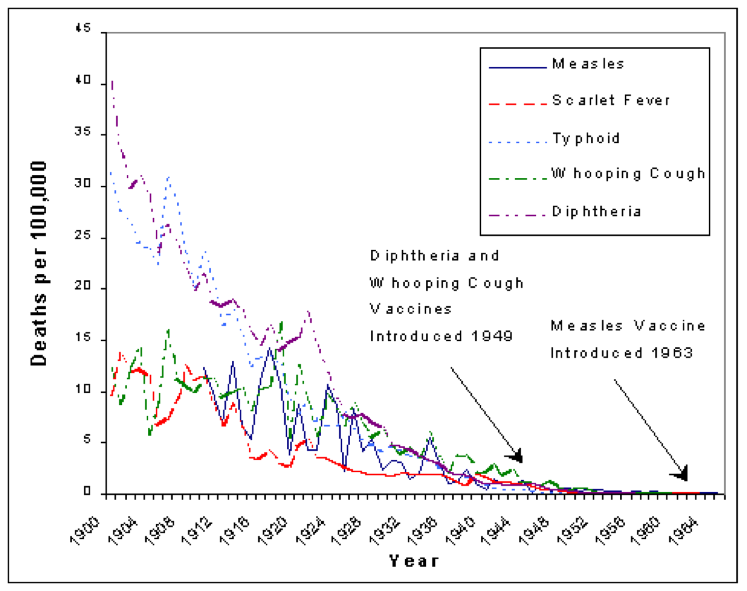
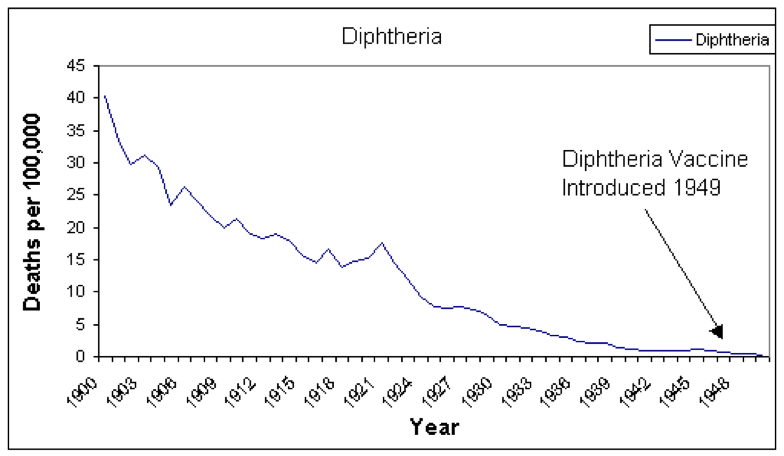
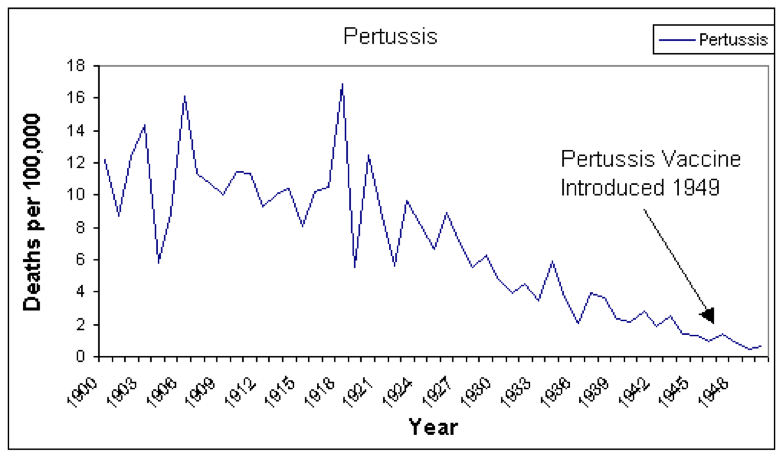
So in effect you are allowing your infant to be inoculated with a pharmaceutical based vaccine to protect the infant from diseases that declined across the planet 50 years ago so with that being said the benefits of protection from a low incidence disease is not very high.
Remember the incidence of Diphtheria in the US between 1980-1999 was 3 cases/year from 1920 where there were 150 cases/year. Pertussis (Whooping cough) incidence in the US as I said above has been rising from 1730 cases in 1980 to 20,679 in 2016.This trend is also mirrored in Australia. In contrast in the UK there were 22.924 cases in 1980 which is reduced to 7,085 in 2016. In Canada in 1980 (2873 cases ) vs 2016 (2895 cases), so nothing much has changed. Tetanus incidence for example between 1995-1997 were 124 reported cases (out of approx 300 million -US Population), of those 66 had unknown vaccination status and 8 died), 27 were unvaccinated and 4 died), 12 had received 1 dose of the tetanus vaccine no deaths, 4 had received 2 doses of the tetanus vaccine and 1 death, 4 had received 3 doses of the tetanus vaccine and no deaths, and 12 had received 4 doses of the tetanus vaccine and no deaths.
We have also known since the 40’s that Good Wound Hygiene is the best way to prevent tetanus..let it bleed a bit (losing 10cc of blood is not going to kill you ), clean it thoroughly and pour Peroxide on the wound to disinfect it (In fact if the wound is severe, you will probably get marched of to the ER. You can get another vaccine called Tetanus Immune Globulin which contain ready made antibodies and can be injected directly into the wound itself..remember next time at the ER refuse the tetanus shot and insist on the TIG).
However, people travel so how much does the risk increase in terms of infection?. The link below is a great spreadsheet showing disease incidence across the world from 1980 to 2016 so you can evaluate your risk anywhere where you might be traveling. For instance a few examples of disease incidence in 2016:
DIPTHERIA PERTUSSIS TETANUS
Australia 8 20,037 7
India 3,380 37,274 3,781
Indonesia 342 826 522
Madagascar 2,865 321 136
Thailand 16 84 61
US 0 20,769 0
Canada 1 3,896 5
UK 1 7.085 4
Ironically the Pertussis vaccination schedule is the same in the US as in Australia and both countries are chalking up 20,000 or so cases in 2016 and in 1980 the US had 1730 cases and Australia had 124 cases. So what is happening ??. Unless both countries have regressed their living conditions, sanitation etc back to the level of the 1920’s there is a distinct possibility that the vaccines and/or the dosage is contributing to the increased incidence rate.
http://apps.who.int/immunization_monitoring/globalsummary/timeseries/tsincidencediphtheria.html
Conclusions
I hope in this article I have given you sufficient information for you to draw your own conclusions in terms of the decision to vaccinate or not. If I were faced with this decision and I lived in the US for example I would want to consider a Pertussis vaccine as a monovalent vaccine (not a 3 in 1 or 5 in 1 vaccine, presupposing this vaccine is available as a single vaccine which I doubt ) since Pertussis is fairly significant, but Tetanus and Diphtheria incidences are almost insignificant. However, if I were planning to travel to India where it seems most diseases still exist in relatively high numbers, I would definitely consider the 3 in 1 for an adult and a child. Depending on the circumstance I believe there could be a reason to vaccinate as I described in my example before. However, if you have no choice but to subject your infant to this barrage of vaccines you should insist that the pediatrician check thoroughly and ensure your child has a ROBUST IMMUNE SYSTEM and a healthy gut flora. If you don’t you are putting your child at risk.
“The conquest of infectious disease and the health revolution it initiated is arguably one of the greatest achievements of Western civilization. Yet the phenomenon is largely unknown and rarely taught, even in history courses. Conventional wisdom usually assumes that conquest of infectious disease can be credited to well-known lifesaving innovations in medicine such as vaccines, antibiotics, and surgical asepsis. These icons are truly essential ingredients of modern medicine, and their contribution to human life and health in this century can never be minimized. However, except for the smallpox vaccination, which was introduced in 1798 and made compulsory in England in 1853, the overall contribution of medical innovations to the health revolution of the 1800s is difficult to validate. Diphtheria, tetanus, and pertussis vaccine arrived on the scene only after disease mortality rates already had been reduced significantly; measles, rubella, and polio vaccines did not become available until the middle of the 20th century, when most infant deaths were the result of other causes. The same holds true for sulfa drugs and antibiotics. Their contribution is unequivocal, but they did not affect mortality rates until the 1940s.”
2001 paper in the Journal of Infection Control
References/Acknowledgments:
- The Vaccine Mom DPaT
- Infant Mortality Rates regressed against number of vaccine doses routinely given: Is There a biochemical or synergistic toxicity N.Miller, G.Goldman 2011 NCBI
- Review of the epidemiology of Diphtheria 2000-2016 Kristie Clarke CDC
- Pertussis cases by year (1922-2015) CDC
- Mortality for Tetanus between 1990-2015: findings from the global burden of disease study 2015 NCBI
- Morbidity & Mortality weekly report (MMWR) Tetanus surveillance US 2001-2008 CDC
- Article archived by Vaclib.org July 2007
- Immunization Monitoring:Total Global Vaccinations reported disease cases WHO
- Dr Sheri Tenpenny on Vaccines R-B Choices Youtube presentations
- Pink Book Pertussis CDC
- Barbara Loe Fisher profile website – Barbara speaks out, Newsletters NVIC
- Vaccine excipient & Media Summary
- State of the World’s vaccines & Immunization 3rd edition 2009 WHO
- 2001 Paper Journal of Infection Control
Author: Eric Malouin