Introduction
This article continues our discussion on psychotropic drugs and sleep disturbance. But first we will walk through the extraordinary events associated with Kenneth Parks.
Kenneth Parks

Kenneth Parks met his future wife when she was on the run from her home, so he convinced her to return home to her parents, which she did, and a romance blossomed between them and they got married. His wife’s parents were eternally grateful for the return of their daughter and even more so by gaining a son-in law that they were already fond of, so the relationship between Parks and his in-laws could not have been better. While married he acquired a gambling problem and had embezzled $32,000 from his employer to settle his gambling debts resulting in his dismissal in March 1987. Added to his gambling problem he had a history of somnambulism,the scientific name for sleepwalking, His mother confirmed a sleepwalking incident when he was 13 and she just caught him climbing out of a 6th floor window, and by all accounts there was a family history of this condition; Park’s grandfather would sleep walk, cook some food and not eat it. While married, Parks was suffering with severe insomnia and anxiety due to his unemployment status and his continual losses betting on race horses. In the early morning hours of May 1987 he drove 23 km to his in-laws house, removed a tire iron from the trunk of his car and entered the house and choked his father in law unconscious and then beat and stabbed his mother in law to death. Covered in blood he drove to the nearest police station arriving at 4:45am and confessed saying “My God, I have just killed 2 people” displaying dissociative analgesia ( experiencing no pain despite injury) although he had cut tendons on both hands.
Verdict & post dispute
After extensive physical examination, sleep tests and EEG results, the experts could only conclude that at the time of the crime he was sleepwalking and Park’s mitigating circumstances ( severe insomnia, anxiety, no motive ), and the fact that there was no mental illness his defence counsel convinced the judge to acquit him. The verdict concluded that this homicide was committed during a non-insane automatism as part of a presumed episode of somnambulism. Although Berit Brogaard in her article “sleep driving and sleep killing,” disputes that Parks was fully asleep when he committed the crime, and to drive 23 km negotiating the drive through various intersections without missing a turn or getting lost is almost impossible if you are semi-conscious. Furthermore, it is possible to awaken a sleepwalker, with the screams and yelling that must have taken place during the altercation, questioning why he did not wake up, and the dissociative analgesia occurred not because he was ‘half asleep’ but it was likely caused by a state of shock or distress. There was also some underlying emotional issues with Parks that date back to his childhood ( parents separated when he was 5, no contact with his father until he was 18, no close relationship with his mother, at 16 the parents moved away and Parks went to live with his grandmother, and he also failed in school. This series of events could have been dormant triggers to his gambling problem, anxiety and insomnia.
Glutamate & GABA (Gamma-aminobutyric acid)

Sleepwalking occurs during deep stages of sleep ( slow brain waves ), and the sleepwalker is normally unaware of any sensory input from their environment. Within the body’s sleep circuitry there exists a ‘gating’ mechanism that blocks input from the cognitive brain to the motor systems. The neurotransmitter GABA (Gamma-aminobutyric acid) inhibits activity of the brain’s motor cortex except for twitching that is witnessed when a dog or a cat are sleeping, and their paws twitch. The primary function of GABA is to prevent stimulation by glutamate, the brain’s major excitatory neurotransmitter. Glutamate is a non essential amino acid and can be readily synthesized in the body from citrate within the citric acid cycle. GABA is synthesized from the combination of Glutamate and pyridoxal phosphate ( active Vitamin B6) using an enzyme glutamate decarboxylase,. In Parasomnia these ‘safety valves’ as it were, dysfunction and the brain sends signals uninhibited to the muscles, so although motor circuits are awake, awareness and cognition of the host are asleep. I wonder if they include ‘sleep crime’ in the Minority report…lol. In the next section we will discuss how REM sleep works in terms of biological circuitry and then to analyze what happens when the host takes an antidepressant SSRI for example.
REM Sleep generation
I will attempt to simplify the complexity of the network distribution within the brainstem, forebrain and hypothalamus that together generates REM sleep, Understanding this intricate neural circuitry is necessary to appreciate how psychotropic drugs influence this mechanism. My apologies for the ‘busy’ diagram below, but I wanted to emphasis the complex ‘circuitry’ involved in REM and NREM sleep cycles.
The current hypothesis suggests that within the brainstem, an area called the Mesopontine tegmentum Locus coeruleus (BLUE SPOT on diagram is where the Pontine control of the REM-NREM cycle resides. The switching mechanism is analogous to a simple ‘Flip-Flop’ mechanism used in electronic circuitry as shown below. In this simple circuit Black = OFF, BLUE=ON If S is ON while R is held OFF, then the O/P (output) is forced high, and stays high when S returns to OFF; similarly, if R = ON while S =OFF, then O/P =OFF and stays OFF when R returns to OFF. In other words a NOR gate ( Not OR) is in affect an AND gate meaning that for either reset or set states to be true (ON) both inputs have to be true or high. So its either Set or Reset not both together.

Within the brain a biological version of this flip-flop circuit dictates REM/NREM or wakefulness. Biologically speaking ( the Flip state as it were ) GABA(REM-ON) neurons located in the Laterodorsal tegmental nuclei (RED SPOT on diagram) inhibit GABA (REM-OFF) neurons located in the Ventrolateral periaqueductal gray ( PURPLE SPOT on diagram) and the Lateral pontine tegmentum (BLACK SPOT on diagram). The diagram also shows a purple link from the Ventrolateral periaqueductal gray to the motor cortex to inhibit motor signals being sent to the muscles. During wakefulness the opposite occurs ( the Flop state ) the GABA (REM-OFF) neurons inhibit the GABA(REM-ON) neurons. During the REM-ON state the Glutamatergic neurons that originate from the Pontine control region ( BLUE SPOT on diagram) projects to the basal forebrain as a regulatory mechanism ( EEG characteristics can be measured here), and the Ventromedial medulla (PINK SPOT on diagram) and spinal cord regulating REM atonia ( muscle paralysis to prevent normal muscle movement during sleep.
 .
.
Another subcircuit of REM Sleep generation is the cholinergic ( acetylcholine) neurons that originate from the Pontine control ( Mesopontine Tegmentum-BLUE SPOT on diagram) that innervate receptors within the Substantia nigra (CORN BLUE SPOT on diagram) and the ventral tegmental region (VTA- CYAN SPOT on diagram) that rapidly fire during REM sleep (REM-ON), while the Monoaminergic ( Norepinephrine) neurons stop firing (REM-OFF), and vice versa for wakefulness (CYAN SPOT link to BLUE SPOT ). REM-ON cholinergic neurons originating from the Pedunculopontine and Laterodorsal Tegmental Nuclei (RED SPOT on diagram) are projected to the Thalamus (GREY SPOT on diagram) into its upper brainstem input to the thalamic relay and reticular nuclei which are active during wakefulness and REM sleep. The Thalamus is a unique relay station ( containing relay cells ) that send sensory impulses from receptors in various regions of the body to the cerebral cortex. Typical sensory inputs would be touch, pain or temperature, but in our case its relaying cholinergic ( acetylcholine) signals to the cerebral cortex to induce REM sleep.
Sleep & Drugs ( ..& rock & roll..lol)

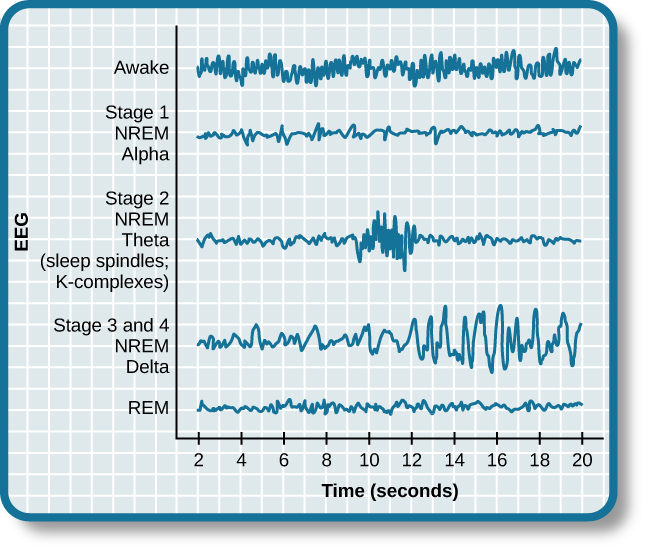
The science has uncovered evidence that Selective Serotonin Reuptake Inhibitors, tricyclic antidepressants ( old antidepressants marketed in the 1950’s largely replaced now with more modern SSRIs) and Serotonin-norepinephrine reuptake inhibitors suppress REM sleep. In addition the anticholinergic properties of individual drugs further disturb normal sleep architecture. The medical profession just love their labels ( nosology) Parasomnia (abnormal sleep related behavior, dreams (???), autonomic changes manifested during transitions from wakefulness to sleep or within transitions between sleep stages ( we have talked about REM and NONREM, but NREM is defined further into sleep stages (SS) :
- Awake stage ( alpha waves )
- SS1,2,3 and SS4 ( delta waves ) and
- REM ( Symmetrical oscillation ).
Typical waveforms of sleep stages are shown below:
Sleep disorders
Other sleep disorder classifications include REM Sleep Behaviour Disorder ( RBD, which is the most common), somnambulism (sleepwalking), sleep terrors ( screaming, intense fear while asleep) which are extreme nightmares especially in children. There is even an exploding head syndrome (imagined loud noises heard when falling asleep or waking up), probably due to Tinnitus ( outer,middle or inner ear problem), catathrenia ( sleep groaning from exhalation ), snoring ( from inhalation), hallucinations, Narcolepsy ( excessive daytime sleeping; affects around 3 million people worldwide) and associated Cataplexy ( brief loss of muscle tone triggered by strong emotions such as laughter; given rise to the expression ‘Weak with laughter’).
Drug induced sleep disorders
The Dorsal Raphe Nucleus ( GREEN SPOT on the diagram) is the largest serotonergic nucleus in the brain and rich in presynaptic serotonin 5 HT autoreceptors that project serotonin signalling to the pedunculopontine tegmental areas ( GREEN SPOT link to the RED SPOT on the diagram above). SSRI antidepressants desensitize the somatodendritic serotonin autoreceptors in the dorsal Raphe Nucleus, amplifying terminal serotonin release inhibiting REM-ON neurons, thus inhibiting REM sleep unnaturally. Since the pedunculopontine tegmental area(REM-OFF cells) has descending projections ( PINK LINES) to the Pontine REM,NREM control (BLUE SPOT on diagram) to activate REM sleep, and to the Ventromedial Medulla(PINK SPOT on diagram) to signal muscle paralysis the SSRI will interfere with these controls as well. It is also suggested that the RBD ( REM sleep behavior disorder ) lesion site is within the subcoeruleus area of the Pontine control. There was a time when science believed that the hypothalamus was the sleep centre of the brain, and wakefulness centre in the brainstem but you can appreciate that regulatory sleep-wake cycles involves a complex interaction of various neurotransmissions within various regions of the brain and brainstem including the circadian rhythmic control provided by the Retina-SCN-PVN-SCG-Pineal-pathway.
Physicians to the rescue
Don’t worry your physician will help your sleep disorder while your antidepressant is ‘curing’ your depression, he can prescribe Trazodone, another antidepressant which is a serotonin antagonist and reuptake inhibitor to help you sleep. I’m confused..so the the original SSRI antidepressant which is inhibiting REM sleep and causing insomnia and God knows what else, you counteract it with taking another drug…so one drug inhibits the reuptake of the serotonin thus allowing the serotonin to hang around longer, while the other drug attempts to suppress it. One of the side effects of Trazodone is INSOMNIA ( not to mention dream disorder, hypotension ( try sleeping with your heart racing ), confusion ( yeah just like me) so how is this drug supposed to help you sleep when it’s having a serotonin fight with the SSRI. Are these doctors taking their own drugs ??…….oh I see now, that’s why the other side effects of Trazodone is night sweats, micturition ( possible bed wetting)…seems reasonable while these 2 serotonin drugs are ‘duking it out’ you end up sweating. What else is there..migraine, agitation ( that’s good for a good night’s sleep), paraesthesia ( abnormal tingling, pricking tickling, numbness or skin burning sensations ( oh yeah just what I need to sleep), and tremor ( that’s what I could do with, a good tremor while I’m trying to sleep).
What is my signature expression?..”take me to the rubber room”
SSRI’s and RBD
SSRI’s also produce ‘Prozac’ eyes, where the victim…I mean patient, experiences rapid eye movement within NREM ( Non rapid eye movement ). This condition is a symptom of REM Sleep Behaviour Disorder (RBD) which as reported in 2007 by Maja Tippmann-Peikert MD a sleep medicine specialist and neurologist where patients will act out unpleasant and violent dreams due to the loss of natural muscle paralysis during REM sleep. Dr Robert Auger another clinical sleep medicine specialist from the Mayo clinic commented after a study analyzing patients (average age 34) diagnosed with a RBD between 2002-2005:
“Although previously published case reports and a more recently published study have suggested the association between antidepressants and RBD, this study represents the first systematic demonstration of the relationship”
Patients were prescribed SSRIs, Venlafaxine (brand name Effexor -Serotonin-norepinephrine reuptake inhibitor), Mirtazapine (Brand name Remeron) and the old tricyclic antidepressants. Dr Auger also stated that :
“A link between antidepressants and RBD is not completely surprising, as the neurotransmitters affected by these medications are involved in REM sleep regulation, and a recent study shows that they diminish the muscle paralysis associated with normal REM sleep.”
Serotonin production working overtime
So it’s clear that SSRI antidepressants inhibit the reuptake of serotonin into the firing synapse of the serotonergic neuron. What results is serotonin firing continuously to the receiving dendritic neuron and the synaptic cleft, interfering with the natural cycle of serotonergic activity during daytime and the serotonin silence during the night. This means the serotonergic system is working 24 hours/day, and its cyclical pattern in harmony with circadian rhythm is lost. This raises the possibility that consciousness may drift closer to a ‘dreamlike state’, causing the person in some instances an inability to distinguish between reality and dreaming. Furthermore if dream states and sleep is being deprived, the brain may hallucinate.
High levels of serotonin
It is hypothesised that high serotonin levels also build up in the pineal gland, since there is evidence to suggest that autopsies performed on dead mental patients found excessive amounts of serotonin in the Pineal. It is further hypothesised that the Pineal gland secretes other serotonin derivatives namely psychoactive derivatives such as Pinoline (6-Methoxy-Tetrahydro-Beta-Carboline) a beta-carboline which is a naturally occurring Alkaloid (Nitrogen based ) like morphine extracted from the Opium Poppy. Tryptamines like DMT (Dimethyltryptamine and 5-MeO-DMT (5-Methoxy-Tryptamine) also have psychoactive properties ( Hallucinatory), and Bufotenine (5-Hydroxy-Dimethyltryptamine) are also thought to be secreted by the pineal but to date there is no scientific evidence of this. If some serotonin derivatives with psychoactive properties do exist in the Pineal gland coupled with excessive amounts of serotonin then its plausible that excessive amounts of these tryptamines could be unleashed into the brain creating hallucinatory effects. In some individuals maintaining high serotonin levels can cause Serotonin syndrome. Dr Felix Sulman in the 1950’s experimented with high serotonin levels and discovered that it is a stress neuro-hormone and subjecting these high levels to rabbits, the most docile of creatures, makes them aggressive. Since the SSRI antidepressant inhibits proper serotonin metabolism, humans become poisoned by the excess serotonin resulting in migraine headaches, hot flashes, irritability, sleeplessness, pains around the heart, breathing difficulty, irrational tension, anxiety and horrifying nightmares. These findings are clearly explained in Dr Ann Blake Tracy’s book ‘Prozac: Panacea or Pandora’, as well as sleepwalk nightmares caused by RBD.
Conclusions
I hope now you have a better understanding toward sleep. Sleep is crucial for health, and deprive yourself of it by taking poisonous psychotropic drugs will only be detrimental to your well being. These drugs have no business being anywhere near a human; they do nothing, but interfere with your natural physiological, biological, and psychological mechanisms bringing you closer to death. In the final subsection of this series I will discuss Opiates like Oxycontin which reached epidemic proportions in the 1990-2000’s and is also problematic today.
Movie Quote Silent Hill
“P. S. R. Parallel Synchronized Randomness. An interesting brain rarity and our subject for today. Two people walk in opposite directions at the same time and then they make the same decision at the same time. Then they correct it, and then they correct it, and then they correct it, and then they correct it, and then they correct it. Basically, in a mathematical world these two little guys will stay looped for the end of time. The brain is the most complex thing in the universe and it’s right behind the nose. [plays drums] Fascinating!”
Movie Quote ‘The science of sleep 2006
References/Acknowledgments :
- Sleep driving and sleep walking Berit Brogaard PHD 2012 Psychology today
- Man Acquitted of sleepwalking murder running for school trustee in Durham 2006 Citynews
- 4 GABA deficiency symptoms you can identify yourself UHN Daily 2017
- How can dreams control your body? The science of sleepwalking Esther Ingis- Arkell 2014 I09
- What does the Thalamus do ? Sally Robertson News Medical Life Sciences
- The Pontine REM switch: past & present Fuller, Saper, Lu 2007 NCBI (Journal of Physiology
- REM Sleep at its core-circuits,neurotransmitters, & pathophysiology Fraigne, Torentali, Snow, Peever 2015 NCBI
- REM Sleep aka ‘Prozac eyes’ 2007 WeeksMD
- Parasomnias & antidepressant therapy: A review of the literature Kierlin, Lottner 2011 NCBI
- Beta-carboline, Alkaloids Wikipedia
- Silent Hill 2006 quotes Great-quotes.com
- The science of sleep 2006 quote Wikiquotes
- SSRIs and the Pineal Gland 2003 Charles Groenendijk