Introduction
In this part, I want to draw your attention to some side effects that are well documented regarding cholesterol lowering drugs (Brand name Statins) and to explain biologically why they occur. I would also like to discuss a genetic anomoly concerning cholesterol.
In case you missed the first 2 articles you can use the links below to check them out:
Decisions..Decisions

I know there are many documented accounts of patients taking HMG-CoA reductase inhibitors or cholesterol lowering drugs who have suffered adverse effects. Many people who take these drugs probably have very little side effects; since we are all individuals these drugs affect people differently, and adverse effects if any, some are tolerable, some are not. It is not just pharmaceutical drugs it is anything that you ingest, some food or supplements don’t agree with everybody. In the grand scheme of things the hundreds of documented cases where patients have even stopped taking the drug because of the side effects probably pale into insignificance compared to the millions that are taking these drugs. However, pharmaceutical drugs do alter physiological processes and interfere with some of the many pathways and most of the time the adverse effects and risk outweigh the purported benefits. I am not on any anti-drug campaign but just to make you all aware that there are far more risks in taking drugs than most food even processed and fast food, and you as individuals must make up your own minds if it is worth taking the risk. If you are eating recklessly without eating at least some nutritional food or health supplements eventually the body is going to send you a signal which may not be very pleasant and if this involves pain you feel inclined to visit your family doctor who will try and help you..that’s his/her job and you are his/hers responsibility to make you feel more comfortable.
Reported Adverse Effects from HMG-CoA reductase inhibitor drugs
The Journal of Independent medical research published a report which was compiled using actual patient accounts of adverse reactions from the HMG-CoA reductase inhibitor drugs. Three hundred and fifty one patient accounts were collated. Every patient reported some adverse reaction and 61% said they had ceased taking them because they could not tolerate the side effects. Sixty three reported that they had sustained permanent damage and 120 were still experiencing unresolved adverse reactions. Eighteen had contracted Amyotrophic Lateral Sclerosis (ALS). Twenty nine had acquired major neurodegenerative disorders including Parkinson’s, Alzheimer’s, multiple system atrophy (also known as Shy Drager Syndrome, a rare condition characterized by tremors, slow movement, muscle rigidity, postural instability balance difficulty), progressive supranuclear polyneuropathy (another rare condition also called Steele-Richardson-Olszewski syndrome causing serious problems with walking,balance and eye movement caused by cell deterioration), chronic demyelinating polyneuropathy (a neurological disorder characterized by progressive weakness and impaired sensory function in the arms and legs caused by damage to the myelin sheath) and ALS (known also as Lou Gehrigs disease which causes progressive muscle weakness and wasting, walking difficulties). Sixty nine experienced memory issues ,18 had some cognitive impairment and 6 had experienced transient global amnesia ( sudden temporary episode of memory loss). This was all reported to the Medical & Health Products Regulatory Agency (MHRA), the UK’s version of the FDA in the US. The problem with studies and reports like this unless there is definite proof that it was the actual cholesterol lowering drug it could have been a potentiation with other medicines or the individual predisposition to the effect, but certainly with these types of drugs one of the major side effects as stated on the drugs.com site is muscle cramps,pain, stiffness, swelling or weakness in in rare cases myopathy (muscle problems), myositis (muscle inflammation) or rhabdomyolysis (damaged skeletal muscle causing rapid breakdown which is also caused by extreme exercise as well).
Blocking the Mevalonate Pathway
The above patient reported adverse effects are documented on many websites, some are rare but have occurred in some individuals, but exactly how people respond depends upon the genetic disposition and faced with any deficiency the body will make its own decisions to sacrifice some cells in order to preserve others; like a backup plan of sorts. In the extreme, in one individual, Alzheimer’s, or ALS may develop where the body sacrifices neuronal cells to protect the heart cells or Rhabdomyolysis may occur to save neuronal cells. More commonly, in most people the adverse effects are less severe causing muscle pain and weakness, and in some case diabetes or sudden temporary memory loss (transient global amnesia).
Let us first look at this pathway which is shown below:
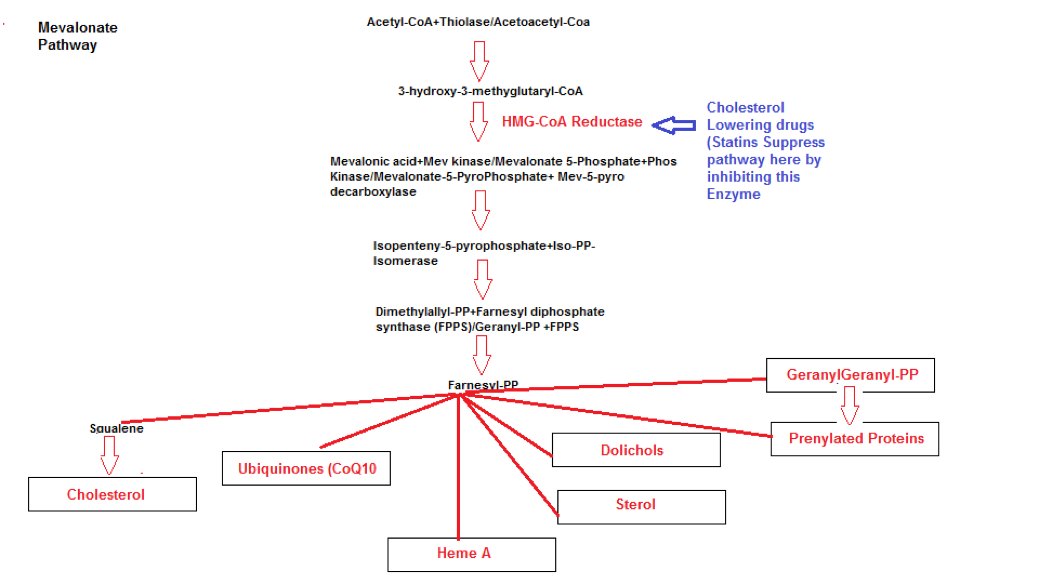
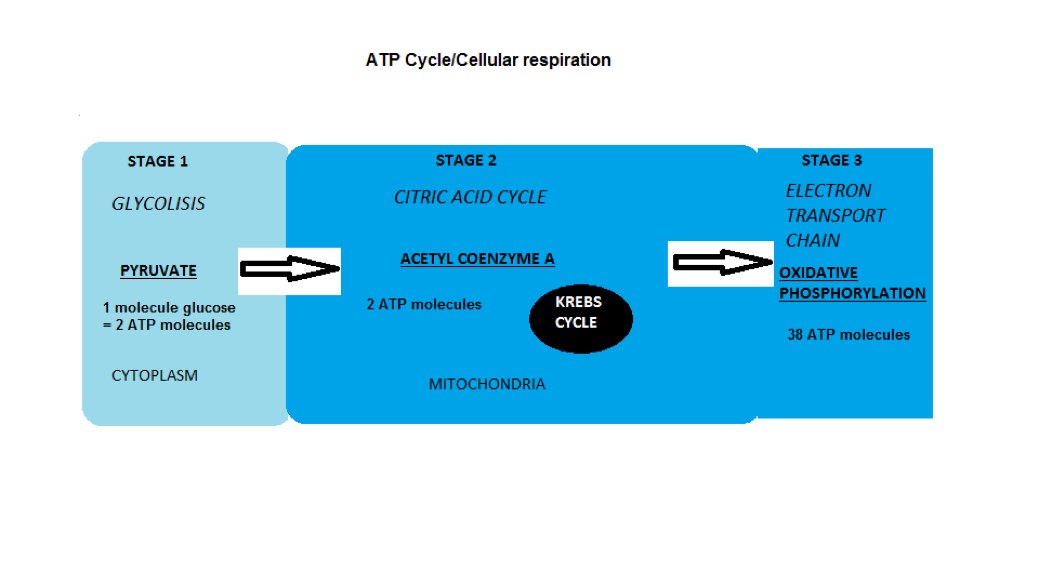
One can immediately see what product are affected by suppression of this pathway namely Cholesterol, Sterol, Dolichols, Heme A, Ubiquinone (Coenzyme Q10) and Prenylated proteins. In the following paragraphs I will attempt to uncover the various consequences in interfering with these products giving rise to the adverse effects that these drugs can unleash in the body. First of all lets us consider basic biology, specifically the mitochondria (organelles) within the cell. This is the cell’s powerhouse where energy is produced. If you have read part 1 of the article series Cancer you will remember the following diagram:
Mitochondria

The Kreb Energy Cycle
We have covered this in an previous article, but basically from the diagram the aerobic energy metabolic process that occurs in every cell is highly efficient achieving movement by burning 1 molecule of glucose which can generate 38 ATP molecules within the mitochondria. In muscle cells especially it is essential that this level of energy is generated while under load conditions such as exercise. Although a small amount of energy is generated in the cytoplasm,without the need for oxygen achieved by anaerobic metabolism via fermentation producing lactate acid occurring within the cytoplasm without the use of the mitochondria. Under certain exercise conditions where your pushing your body to the limits, your muscles may start to hurt because the oxygen to the muscle has been depleted and your cells have reverted to anaerobic respiration. In any event muscle movement when exercise requires maximum generated ATP energy from the electron chain transport process.
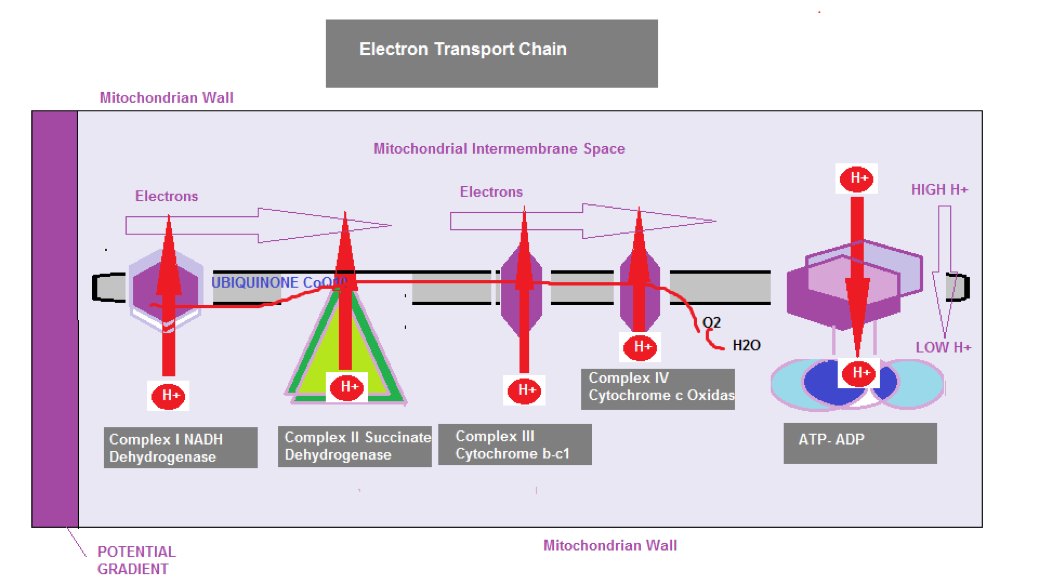
The Electron Transport Chain
In stage 3 (from the diagram below) the electron transport chain working within the inter-membrane space of the cell, is the final stage of cellular respiration called Oxidative Phosphorylation which involves the electron transport chain and Chemiosmosis. The electron transport chain passes electrons between molecules and it is these electron transfers that produce an electrical proton gradient moving from a higher to a lower energy level by injecting hydrogen ions(H+) into the membrane space creating a battery like differential charge across the membrane (Potential Gradient) Chemiosmosis is the energy stored in the gradient and released as ATP energy.
Coenzyme Q10 Insufficiency
An antioxidant Coenzyme Q10 (described in the next section) is used to maintain functional efficiency of the chain, but if there is a reduction in CoQ10, these H+ ions will begin leaking into the mitochondria causing dysfunction in the chain. Oxygen sits at the end of the chain accepting electrons and the hydrogen ions thus forming water (H20), however if the process dysfunctions it will have an effect of insufficient oxygen ( although oxygen is present ) which is only partially converted to water, due to the leaky H+, leading to the production of toxins, like Hydrogen Peroxide, so the whole process slows down due to the lack of Coq10, causing a decrease in ATP generation and the muscles can’t keep up with demand and the muscles become weak and painful. This effect is synonymous to extreme exercise like a marathon or impact training where your body becomes oxygen and glucose depleted and as stated before energy production will switch to anaerobic respiration via a fermentation process but the ATP output is only 1/16 as it would be from the kreb cycle in the mitochondria. Although lactic acid is being produced and poured into the bloodstream acting as an alternative fuel source for the heart, but ultimately though, fatigue and muscle aches will set in quickly if the exercise is maintained at this extreme level. There is slightly more to this story, such as the glucose alanine cycle but is not relevant to discuss here, but this gives you a scientific overview toward why HMG-CoA reductase inhibitor drugs cause muscle pain and weakness.
Rhabdomyolysis
The New York times in 2002 in an article entitled ‘Personal Health; Statins: Miracles for some, Menace for a few reported that in August 2001, Bayer voluntarily recalled their statin drug Cerivastatin ( marketed as Baycol) because it had caused the death of 31 people from Rhabdomyolysis. The article went on to recall an 82 year old Kansas woman who had been taking statins for a number of years and for the entire time she experienced muscle pains. She even underwent an unnecessary shoulder operation to try and cure the drug induced pain. Then she was treated with an antifungal agent for skin lesions that her physician failed to diagnose as a result of the drug induced muscle breakdown. The tragic combination of antifungals and statins worsened her condition to the point where she could not stand or breathe on her own and she was dead in 3 months (why didn’t anyone stop the statins ???).
Rhabdomyolysis is a rare side condition of cholesterol lowering drugs, nevertheless the risk exists. This condition describes rapid muscle disintegration which is commonly fatal because it causes acute renal failure. The reason for this is the substance Myoglobin an iron/oxygen binding protein found in muscle tissue (actually myoglobin exists to help muscle cells to store oxygen, and to transport oxygen from the cell walls to the mitochondria). Related to hemoglobin, this protein is only found in the blood after muscle injury that slough this substance off in large amounts which then get filtered through the kidneys. However,this substance is a protoxin (a toxin precursor, since myoglobin is Mg+2 Ferrous, its normal form, but if it takes on 2 extra protons it becomes Mg +4 Ferryl which is toxic and cause peroxidative damage to the kidney cell wall) to the renal tubular epithelium (cells that make up the renal tubule which is part of the Glomeruli first stage filtering process used for urine excretion) which may result in acute kidney injury or failure, due to kidney overload. There are over a million nephrons in each kidney so the renal tubes are miniscule which are designed for fluids not large amounts of myoglobin, which can block the renal filtration system. It is the interaction between the myoglobin and mitochondria of the kidney cells, that causes the mitochondrial membranes to become oxidized, leading to cell death. This problem manifest itself when excreted urine becomes the color of tea. Physicians can test the blood looking for high levels of creatine kinase* which will indicate kidney damage but the tea colored urine is a dead giveaway.
* Creatine kinase is an enzyme that catalyses creatine a nitrogenous organic, a compound that is generally synthesized in the liver and kidney for the purpose of ATP recycling by creating Phosphocreatine (Pcr) that serves as a reservoir for rapid re buffering and regeneration of ATP.
Coenzyme Q10 (CoQ10)
A crucial substance is produced to assist energy production specifically at the back end of the Electron Transport chain (final stage 3 in the diagram). This substance is Coenzyme-Q10 (CoQ10) and it has a dual function, as a mobile messenger link and an antioxidant. Each pair of electrons processed in the chain have to interact with CoQ10 (this interaction can be visualized in terms of considering the cell as an engine using oxygen to burn organic fuel from food and CoQ10 is the spark plug for the engine, without Coq10 no energy is produced.) As CoQ10 is an energy carrier so to speak, it continuously goes through an oxidation-reduction cycle. When it accepts electrons it becomes reduced (normal state) and when it gives up an electron it oxidizes. From the previous section on Rhabdomyolysis, we mentioned that myoglobin builds up in the muscles and ends up as a toxic substance that causes oxidative damage to kidney cells and the buildup of hydrogen peroxide within the electron transport chain. Both instances could be contained with sufficient Coenzyme Q10. This is the reason that physician should prescribe CoQ10 to their patients who decide to take these cholesterol lowering drugs (I noticed that some studies refute the need for CoQ10 supplementation, but you only have to understand the science to appreciate the plausibility of its usefulness)
Cholesterol
We also discussed the main enzyme HMG-Coenzyme A Reductase which the body activates to manufacture cholesterol in the liver and cells throughout the body. The body is intelligent enough to know when to activate this enzyme and when to simply turn it off. The body regulates cholesterol in the body and senses hormonal signals like Insulin, although, we all know is a hormone signal to trigger cellular uptake of glucose from the blood, but it also turns on HMG-Coenzyme A Reductase to signal the cells and the liver to make more cholesterol even if it is not required. If you continue to consume excess refined sugar and processed food etc the insulin level will remain high causing eventual cellular insulin resistance and excess cholesterol. The reason for this is, high Insulin tricks the body into a request for growth at the cellular level. It is another reason why the human body is not designed for excess sugar and starch consumption, and why serum cholesterol increases. In summary therefore refined carbohydrates speed up the cholesterol assembly line and cholesterol lowering drugs slow the cholesterol assembly line. It also proves that cholesterol production can be controlled by diet. Just to be sure you understand these drugs are inhibitors so they don’t stop the mevalonate pathway process they simply slow it down, if they did block it completely individuals would not survive, not even on a high cholesterol diet.
Familial Hypercholesterolemia (FH)
According to the documented research, FH is a genetic disorder ( Autosomal dominant pattern) that appears in 2 modes Heterozygous ( where only one gene is abnormal), and Homozygous ( both genes are abnormal) that causes High serum cholesterol levels.
Statistically, Heterozygous gene abnormality occurs in 1 in 500 people in most countries and Homozygous gene abnormality afflicts 1 in a million. Nessa Carey in her book ‘Junk DNA’ reports that in the UK approx 120,000 people ( total population approx 60 million) live with FH , while about 1/3 to 1/2 of the FH sufferers end up with coronary artery disease by their mid 50s. These figures show that FH and its severity, varys.
Furthermore, according to Wikipedia, FH is classified as type 2 familial dyslipidemia. Type 2 refers to LDL receptor dysfunction caused by the abnormality of the gene, that defines the protein(s) necessary to produce the necessary number of LDL receptors to remove LDL particles from the serum, and this gene is called the LDLR gene.
The type 2 FH has 5 classifications where one classification is associated with PCSK9 ( Proprotein Convertase Subtilisin/Kexin type 9), a protein involved in transporting fat molecules ( incl Cholesterol) by binding to LDL particles from extracellular fluid into the cell, reducing LDL particle concentration.
A drug called PCSK9 inhibitor are used to block the PCSK9 gene which causes more LDLRs to be recycled, in other words it blocks the protein production that regu;ate the amount of cholesterol produced by controlling the number of LDL receptors. However PCSK9 is responsible for lipoprotein homeostatis, and in clinical trails there was evidence that their use heightened the risk of cognitive disorders.
Another classification is associated with an Apolipoprotein ( B in its ApoB100 form) that is involved with binding to the LDL receptor that is reduced by the mutancy since Glutamine is produced instead of Arginine.
At first glance the choice of a Statin drug in this special FH condition is the perfect choice. As we explained in Part 2 the rate limiting step in cholesterol synthesis is regulated by the membrane protein enzyme HMG-CoA reductase that catalyses this step in converting HMG-CoA into Mevalonate.
HMG-CoA is sterol sensing in order that they can down regulate HMG-CoA reductase when cholesterol levels are high. This down regulation of HMG-CoA reductase is achieved by the interaction of Lanosterol accumulation in the membrane of the Endoplasmic Reticulum ( ER)( An area within the cell responsible for protein processing) that binds with another protein Insig within the cell.
If there are an inadequate number of LDL receptors being produced to take up the excess serum cholesterol, the next best thing is to limit the amount of cholesterol synthesis being produced in the first place.
The Statin drug works on the basis of molcular mimicry of HMG-CoA where it competes for binding to the HMG-CoA reductase thus inhibiting the actual biological HMG-CoA reductase, and slowing down the mevalonate pathway.
The question now is, if the membrane domain HMG-CoA reductase is sterol sensing, and cholesterol levels are high would the down regulation of this enzyme not be enough to maintain appropriate cholesterol level ?.
The same cellular feed back circuitry functions if cholesterol levels are low, by increasing the the biosynthesis of cholesterol, HMG-CoA reductase and proteins that increase the uptake of cholesterol from the external environment i.e LDL receptors.
Bergamot Orange a possible natural therapy to treat Dyslipidemia
It would appear that the existing research does not address this question since the bias is toward the use of Statin drugs, but Cardiologist Stephen Sinatra has put together a formulated product that incorporates Bergamonte ( a small citrus fruit that grows in Calabria Italy called a Bergamot orange that tastes more like a lemon and used to flavor Earl Grey tea).
Most citrus fruits contain flavonoid phytonutrients, but the Bergamot is extremely rich in these health promoting substances consisting of O-Glycosides and C-Glycosides ( these occur naturally in flavonoids which tend to feed our gut bacteria in the small and large intestines ).
Examples of O-Glycosides are Neoeriocitrin (Antioxidant that prevents oxidation of LDL Particles), Naringin (Anti-Inflammatory) and Neohesperidin, Brutieridin (Inhibits HMG-CoA Reductase), Melitidin(Inhibits HMG-CoA Reductase), Rhoifolin 40‐O‐glucoside, chrysoeriol 7‐O‐neohesperidoside‐40‐O‐glucoside, diosmin, rhoifolin, chrysoeriol 7‐O‐neohesperidoside, narirutin, and neodiosmin.
C-Glycosides include apigenin 6,8-di-C-glucoside, diometin 6,8-di-C-glucoside, lucenin‐2, vicenin‐2, stellarin‐2, lucenin‐2‐40‐methyl ether, scoparin, and orientin 40‐methyl ether.
Flavonoid C-glycosides significantly show antioxidant activity, anticancer and antitumor activity, hepatoprotective activity, anti-inflammatory activity, anti-diabetes activity, antiviral activity, antibacterial and antifungal activity, and so on.
Most of the time C-glycosylflavonoids show higher antioxidant and anti-diabetes potential than their corresponding O-glycosylflavonoids.
Outcomes of Bergamot studies
It is acknowledged that oxidised cholesterol can damage the arterial epithelium, possibly leading to the accumulation of debris in and along the arterial wall producing an atherosclerotic environment compromising blood flow. Studies such as ‘Antioxidant activity of citrus limonoids, flavonoids, and coumarins’Yu J et al conducted in 2005, identified the antioxidant power of Naringin, Neoeriocitrin, and Rutin contained in the Bergamot fruit lowered LDL particle oxidation.
Another study ‘Naringin has an antiatherogenic effect with the inhibition of intercellular adhesion molecule-1 in hypercholesterolemic rabbits’ conducted by Choe SC in 2001 compared Naringin and Lovastatin showing a reduction in fatty streak formation and macrophage inflitration in endothelial cells (Endothelium) that line the interior of blood vessels and Naringin, but not Lovastatin, had a hepatoprotective effect ( preventing liver damage).
Injured blood vessels and Neointima formation ( arterial scarring) that occur after angioplasty procedures ( arterial stent implants) have also been shown to be reduced in rats after a 14 day administration of Bergamot oil.
A study was conducted in 2009 by Di Donna et al called ‘Statin-like principles of bergamot fruit (Citrus bergamia): isolation of 3-hydroxymethylglutaryl flavonoid glycosides.’ proposed that Bergamot compounds Neohesperidin and Naringin share similar chemical structure to statins.
A computational modelling study ‘On the inhibitor effects of bergamot juice flavonoids binding to the 3-hydroxy-3-methylglutaryl-CoA reductase (HMGR) enzyme’ conducted by Leopoldini M, et al in 2010 confirmed Bergamots statin-like molecules bind to the HMG-CoA compound.
Another study divided 3 sets of rats where group1 was fed a normal diet (control group), group 2 was fed a high cholesterol (hypercholesterolemic ). and group 3 the same hypercholesterolemic diet + 1ml of bergamot juice daily, for 30 days.
The third group who received the Bergamot juice ( measured 370 ppm of neoeriocitrin, 520 ppm of naringin, and 310 ppm of neohesperidin) had reduced levels of cholesterol (29.27%), triglycerides (46.12%), and LDL (51.72%) and an increase in HDL (27.61%).
The Atherogenic index of Plasma ( AIP ) is claimed to be able to predict cardiovascular risk by calculating the Log of Triglyceride value/HDL cholesterol value measured in mmol/L or mg/dl. If the resultant AIP value is <0.11 then risk is low, if it is between 0.11 and 0.21 then the risk is intermediate, and if it is >0.21 then the risk is high. In this experiment AIP = 1.09 ± 0.10 for group 3 compared to 3.09 ± 0.20 for group 2.
Finally, a randomized double-blind placebo-controlled study ‘Hypoglycemic and Hypolipemic Effects of a New Lecithin Formulation of Bergamot Polyphenolic Fraction’ conducted by Mollace V et al in 2018 involved three randomized groups totalling 20 patients with varying levels of Hyperlipidemia, with average measured values of LDL cholesterol > 120 mg/dl and triglycerides > 175 mg/dl, and serum glucose > 110 mg/dl. in each group, Placebo, Bergamot polyphenol fraction (BPF) and Bergamot polyphenol fraction phytosomal formulation (BPFP).
The BPF group received 2 * 650mg daily doses of the extract formulation, and the BPFP group received 500g twice daily, both groups for 30 days. The BPF group’s total cholesterol diminshed from 262 to 196, LDL cholesterol from 175 to 116, and triglycerides from 252 to 170.
Similar results were seen with the BPFP group total cholesterol from 261 to 198, LDL cholesterol from 174 to 113, and triglycerides from 252 to 173.
Prior to this study in 2015 ‘Bergamot Reduces Plasma Lipids, Atherogenic Small Dense LDL, and Subclinical Atherosclerosis in Subjects with Moderate Hypercholesterolemia: A 6 Months Prospective Study.’ conducted by Toth PP, et al using 80 patients (42 male, 38 female) with moderate Hypocholesterolemia ( 160-190 mg/dl), who received 150mg each per day for 6 months decreased total cholesterol from 255 to 224, LDL cholesterol from 159 to 132, and triglycerides from 159 to 133, and an increase in HDL from 50 to 54.
Conclusions
So we have uncovered the reason why Statin cholesterol lowering drugs cause muscle pain and in some rare instances Rhabdomyolysis by understanding how these drugs affect mitochondrial activity in energy production in terms of causing Cholesterol and Ubiquinone deficiency.
From various studys on the Bergamot citrus fruit, it has shown that administration of its juice and extract has a profound effect on the lipid profile of patients suffering from Hypercholesterolemia. In the next part we will discuss what happens when the other products Sterol, Dolichols, Heme A, and prenylated proteins are suppressed.
So, finally, a class of drugs had been found that lowered cholesterol levels, protected against heart disease, and didn’t kill people at the same time – hallelujah! ‘On this basis, I put it to the members of the jury that the cholesterol hypothesis had been proven, beyond doubt. This court must convict cholesterol of crimes against humanity, m’lord:
Judge (placing black cap on his head): ‘I order that this sad and dangerous chemical be taken from this place, to another place, where it shall be hanged by the neck, until dead. May God have mercy on its soul.”
Quote from the Book ‘The Great Cholesterol Con’ Dr Raymond Kendrick
References/Acknowledgments:
- The cholesterol myth Book by George Mann MD
- The great cholesterol con Book 2008 by Dr Malcolm Kendrick
- Coenzyme-Q10 Michael Schachter Center for Complementary medicine
- STATINS Drugs.com
- Multiple system Atrophy, Myoglobin, Electron Transport chain, Creatine Kinase Wikipedia
- Statins and Myoglobin: How muscle pain and weakness progress to heart, lung and Kidney failure 2010 Paper authored by Stephanie Seneff MIT
- Familial Hypercholesterolemia Wikipedia
- Cellular control of cholesterol Peter Takizawa Dept of Cell biology Yale
- Diagnosis :Diet Cholesterol Georgia Ede MD
- Statins : Sugar coating the truth Tuit Nutrition 2015
- AIP Calculator Milada Dobiov http://www.biomed.cas.cz
- Clinical application of bergamot (Citrus bergamia) for reducing high cholesterol and cardiovascular disease markers 2019 Mireille Nauman & Jeremy Johnson NCBI (PubMed)
- Statins SpaceDoc Dr Duane Graveline
- Personal health statins: Miracle for some, Menace for a few New York Times Article Jane Brody Dec 2002
Author: Eric Malouin