Introduction
How many reading this article has lost a relative to this disease?
I lost 2 uncles and an aunt, a grandfather and my second wife who had metastatic cancer which began in the brain and progressed to her bones, liver and brain. I believe most people share the same tragic story.
Fear among most people is the word “Cancer” because they know chances of survival in most cases is minimal.
There are however life extension modalities from conventional medicine’s limited arsenal of chemotherapy drugs, radiation and surgery.
Some actually have been curative for a while. For example Chemotherapy applied at an earlier diagnostic stage of some blood cancers like hodgkin’s lymphoma and leukemia has resulted in a ‘temporary cure.
Even surgical procedures to remove prostate glands with localized tumors have cured the patient.
Some modern cancer drugs that are based on a monoclonal antibody process that acts as a GPS for chemotherapy treatment specifically targeting tumors is a definite improvement to the old drugs that just poisoned and destroyed everything, cancer and healthy cells alike.
But after 50 or 100 years in our modern era, has cancer been defeated?
In an effort to uncover the truth behind cancer it’s necessary to explain some very significant historical periods within the last 100 years. As they say in the movies:
“What you are about to read is based on actual events – but not necessarily in chronological order”
Efforts to Find the Miracle Cure

In 1980, ‘Interferon’ was introduced to the world as a possible means to treat cancer successfully. Interferons are signaling proteins or Cytokines that I mentioned in the articles dealing with the ‘microbiome and the immune system’. These interferon cytokines mobilise the immune system’s NKC (Natural killer cells) and Macrophage rank and file.
The interferon drug was a man made synthesis of the cytokine that is naturally made in the body. In 1980 it was published in the medical journals of the day as an immune stimulant that would bring cancer to its knees, but unfortunately it did not.
Then in 1985, another ‘miracle cure’ was found, Interleukin 2, another immune stimulant, that did not work either.
Let us step back a tad and try to understand these various immune system stimulants. First, both Interferons and Interleukins are types of Cytokine as mentioned above, however, these cytokine immune stimulants have one or more responsibilities.
The Interferon provides a barrier between host cells and viruses so as a virus cannot inject its DNA into a host cell for reasons of replication (As they are designed to do in Genetic modification..ref: article Microbiome and the disease Part 2), and they mobilise macrophage cells to absorb viral agents.
The interleukin family of immune system messengers are produced by the leukocyte white blood cells for purposes of immune system regulation.
It was Dr. Steven Rosenberg, now aged 75 is still very active in his research to find a true cure for cancer, and in 1985 he introduced Interleukin 2, where in both preliminary trials like Interferon, had worked their ‘miracle’ magic toward metastatic melanoma and kidney cancer.
In 1992, the FDA finally approved Interleukin 2 as a drug to treat cancer, but in late 1998 a clinical study demonstrated that it didn’t work any better than a placebo. Unfortunately, Interleukin 2 suffered the same fate as Interferon and migrated into the annals of ‘Mythology’.
Within this same period as the Interleukin 2, approval and fateful clinical study, ‘Bone marrow transplants’ were being discussed, especially for breast cancer. Insurance companies at the time refused to reimburse such a procedure due to its unproven status and the immense cost of $500,000.
This opened up a hornets nest, and oncologists began filing lawsuits against insurance companies accusing them of being heartless bullies, depriving women of possible life saving treatment, suffering from aggressive breast cancer who could potentially be saved.
One lawsuit involved Nelene Fox, a 38 year old who developed breast cancer in 1991. Her HMO (Health Maintenance Organisation) insurance company Health Net refused to pay for the bone marrow transplant. She took the matter through the courts and was awarded $77 million in punitive damages, $12 million in compensatory damages and $212,000 in medical expenses.
The reason for Health Nets refusal to pay for the transplant procedure was the advise given by Dr. Sam Ho, medical director of the company, who had been advised himself that the procedure was unproven for advanced metastatic breast cancer.
As it turned out he was right, because the woman was dead two years later in 1993. Nonetheless, the medical profession refused to withdraw the procedure and when Linda McCartney was diagnosed with the same disease in 1995. She too was given a bone marrow transplant in 1998 and within 3 months she was dead.
Two years later, having administered this procedure on 40,000 people with at least 30% who actually died from the procedure itself, the medical community conceded and withdrew it as an acceptable clinical procedure.
 Bone Marrow transplantation is an aggressive procedure that involves removing some healthy bone marrow cells, administering large doses of Chemotherapy drugs (much larger than normal) to destroy completely, the bone marrow in order to rebuild it using the healthy bone marrow initially removed.
Bone Marrow transplantation is an aggressive procedure that involves removing some healthy bone marrow cells, administering large doses of Chemotherapy drugs (much larger than normal) to destroy completely, the bone marrow in order to rebuild it using the healthy bone marrow initially removed.
Unfortunately, in ‘wiping out’ the bone marrow there is a distinct possibility that some of the cancerous cells will resist the chemotherapy onslaught and begin growing back ,but in a more aggressive form.
However, in the case of Linda McCartney the cancer had developed in the liver as well.
Shifting Focus to Angiogenesis
Then Dr Judah Folkman came into the cancer spotlight having studied angiogenesis of Cancer tumors since 1970. Angiogenesis or in this case anti-angiogenesis Folkman theorised that 3 pivotal survival points existed for cancer tumors to thrive:
- Tumors require blood to grow (as all cells..no surprise there)
- Tumors hijack the host to supply themselves with blood
- To hijack the blood supply the tumor secretes hormone like growth factors

In Folkman’s laboratory, one of Folkman’s staff Michael O’Reilly discovered 2 endogenous anti-angiogenic inhibitors Endostatin and Angiostatin, which are proteins that are thought to balance regulation between pro and anti-angiogenic activity outside epithelial and endothelial cellular structures. As a result of his work with mice, in 1998 using an Endostatin drug, he announced that:
“We have not seen a tumor we cannot regress.”
Gina Kolata reporter at the New York times said: “Judah is going to cure cancer in 2 years.”
Even Richard Klausner (Director of the NCI) announced: “I am putting nothing on a higher priority than getting this into clinical trials.”
Even Kolata bounced the idea of a book with her agent, who immediately requested a book advance of $2 million. However, this idea was dropped. The NCI fast tracked a clinical study enrolling some 70 participants in 2006. After the initial uproar of excitement everything went silent.
Then the truth emerged, only 42 participants with advanced pancreatic endocrine tumors or carcinoid (Intestinal or bronchial regions) tumors were recruited, and not one responded to the drug.
In 2 years, Folkman would be dead from heart failure.
Despite the failed clinical trial, Genentech (Roche) manufactured an anti-angiogenesis drug ‘Avastin‘ costing $10,000/month that received approvals in 2004 and 2006, but in 2010 the approval to use Avastin for Breast cancer was withdrawn from the FDA citing that the drug proved ineffective for this type of cancer.
The Hypothesis of Dr. Otto Warburg
Dr. Warburg (1883-1970) was a biochemist who became an MD in Heidelberg in 1911, and studied the metabolism of cancer tumors and the respiration of cells, and in 1931 was awarded the Nobel prize for his discovery of a respiratory enzyme oxidase that orchestrates electron transfer across the cells.
 Warburg postulated that it was the disruption of cell respiration that was the primary cause of cancer and substances like poisons, microbes, radiation, and viruses attributed to a secondary cause of cancer impairing the cell’s ability to breathe. This means that under normal circumstances when we breathe, our cells breathe, i.e inhalation/exhalation of oxygen.
Warburg postulated that it was the disruption of cell respiration that was the primary cause of cancer and substances like poisons, microbes, radiation, and viruses attributed to a secondary cause of cancer impairing the cell’s ability to breathe. This means that under normal circumstances when we breathe, our cells breathe, i.e inhalation/exhalation of oxygen.
If we stop breathing or oxygen runs out we produce lactic acid and over a period without oxygen the cells will begin to ferment sugar from the glycolysis process to survive. So he concluded that that tumor cells survived by the anaerobic metabolism of glucose or fermentation. This was the correct analysis.
Oddly, Josef Issels, a German physician (1907-1998) who introduced the Issels treatment which included the removal of any metal filling from teeth, the elimination of alcohol and coffee, enzymatic therapies, special quackzenes, chelation and nutraceutical supplementation (Laetrile and Vitamin C), made claims that his treatment could be used for cancer.
Issels was arrested for these ‘false’claims and Warburg testified on Issels behalf and Issels was found not guilty.
Issels treatment, which he perfected in the 50’s, was designed to be used as an adjunct to conventional chemotherapy and radiation, to rebuild the immune system that these poisons compromised.
Although he died in 1998, his wife continues to promote his treatment, however, it is doubtful that this combination of natural and conventional treatments for anything would ever work, since allopathic medicine regards natural approaches to the body as a ‘dark art’ claiming that natural treatments simultaneously administered, alongside chemotherapy drugs, interfere with the receptor sites for their poison to be absorbed. This by the way is false,
Warburg’s Hypothesis Today

Energy is generated in every cell in the form of Adenosine Triphosphate (ATP).
Our fuel (food) and corresponding nutrients are taken up by our cells.
This ‘food’ is gradually oxidised in the cell to reform ATP as stored energy in both the cytoplasm and the nucleoplasm.
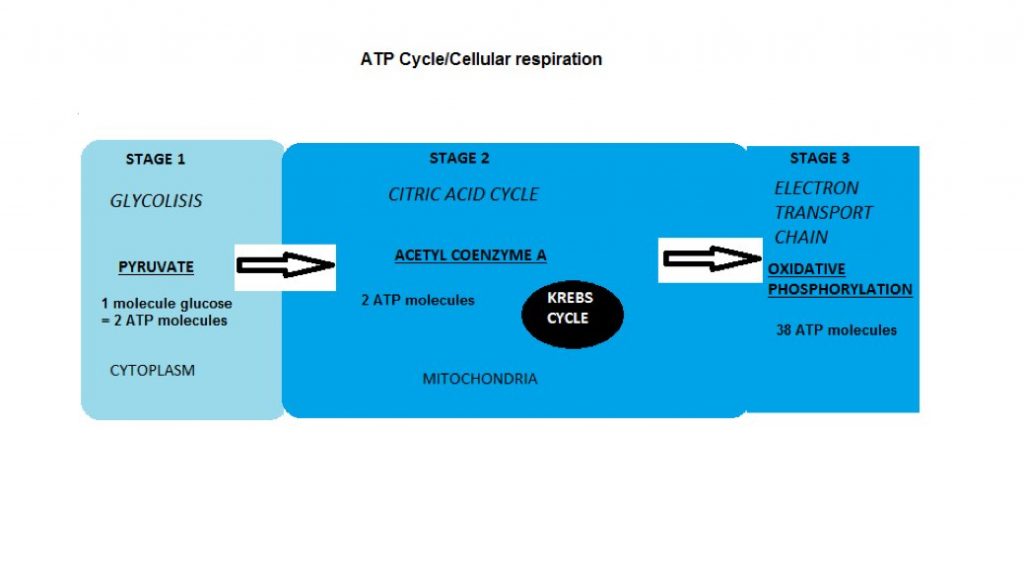
First of all ATP is synthesised in the mitochondrial energy factories by Glycolysis ,a FIRST STAGE process of cellular respiration that metabolises glucose and produces Pyruvate (Pyruvic acid), that junctions between anaerobic (without oxygen) or aerobic (with oxygen) pathways producing a small amount of energy.
In the natural process, if oxygen supply is depleted within muscle cells due to extreme exercise for example, the anaerobic pathway is used to produce lactic acid continuing the ATP energy cycle.
The SECOND STAGE is the Citric Acid Cycle also known as the Tricarboxylic Acid (TCA) or the Krebs cycle which is fed by the Pyruvate that is oxidised to produce Acetyl Coenzyme A to produce more energy from carbon dioxide and water.
This process is catalyzed by enzymes to regulate the cycle (kind of speed control depending on the requirements of the cell’s energy needs). Theoretically the first stage Glycolysis does not require Oxygen, the second stage (citric acid cycle) that occurs in the mitochondria of the cell does need oxygen.
The THIRD STAGE of cellular respiration that also occurs in the mitochondria, takes the electron carriers from the citric acid cycle and deposits them into an electron transport chain to the Oxidative Phosphorylation metabolic pathway for the cells to use enzymes to oxidise nutrients and ultimately release much more energy than the first 2 stages.
Warburg’s theory suggested that cancer cells can only exist in an anaerobic environment, in a fermented state, since it detaches itself after the first stage of Glycolysis from the Citric acid cycle and Electron transport chain.
 The Work of Dr Thomas Seyfried
The Work of Dr Thomas Seyfried

Doctor Thomas Seyfried, professor of biology, at the University of Illinois points out that the current thinking, as it has always been, even before the human genome project, and certainly before our knowledge of epigenetics, is hinged upon genetic mutation.
We know that gene mutations do exist but they are rare.
Humans are ‘diploid’ organisms, that is to say that we receive 2 copies of the same gene from our parents.
These genes can be the same and their ‘Alleles’ (a variant form of a gene ) can be the same or different.
These matching genes from each parent occur at the same location on homologous (chromosome pairs) chromosomes. If both copies are the same then the allele are referred to as ‘Homozygous’, and if one copy is different then the allele is referred to as ‘Heterozygous’.
I am not going into explaining the theory of inheritance or Gregor Mendel’s pea plant breeding and the use of Punnett squares. Suffice to say that, even if scientists believe that human organisms decision to choose which gene copy is based on dominance versus a recessive ‘phenotype’ *, than gene mutation makes sense.
Given the intelligence of the body, it would be more logical that the decision is also based on the biological integrity of the gene, since the driving force of human life is procreation; the continuance of life itself.
During the so-called reproductive years, everything is ‘firing on all cylinders’ but as we age and go beyond the reproductive years (our usefulness to reproduce is over..boo hoo) the human organism begins to degrade; we can slow the degradation down, but we cannot halt or reverse it.
*Genotype and phenotype are two fundamental terms in the science of genetics. … An organism’s genotype is the set of genes in its DNA responsible for a particular trait. An organism’s phenotype is the physical expression of those genes. When the both genes code for the same version of a trait the phenotype will match the genotype. … If, however, the two genes carry different variations for the trait, the phenotype will be determined by the dominant gene. For example, the gene for brown eyes is dominant while the gene for blue eyes is recessive. or a recessive inherited trait is a smooth chin, as opposed to a dominant cleft chin.
Conventional medicine, because they do not fully understand cancer, and how to halt its progression, they create innovative ways to analyze the condition through personalized medicine techniques using clinicians to analyze hundreds of cell mutations taken from tumors in an attempt to identify what drugs to use.
Their dedicated ‘zeal to heal’, hampered by the knowledge that they will always be on the side of treatment, as opposed to prevention, genetics is still the driving force. So how can you possibly deal with inherited Oncogenes (or mutated genes)?
Dr Seyfried questions this ‘dogma’ of genetic disposition when studies like the cloned embryo in a mouse, that is perfectly formed from the implantation of a brain tumor cell.
As he further indicates, a normal cytoplasm (the jelly like aqueous fluid within the cell that separates the cell membrane from the nucleus) together with a tumorous nucleus will divide into a normal healthy cell, while a normal nucleus together with a tumorous cytoplasm produce tumor cells.
His findings, and findings of other scientists are incompatible with the somatic mutation theory of cancer.
In essence Dr Seyfried has embraced the work of Otto Warburg, and proven by mitochondrial analysis, that the mitochondria of a normal cell contains inner membrane folds known as ‘Cristae’ that store the cells energy, whereas in a tumor cell the mitochondria is empty having no energy storage but simply surviving on fermented glucose as opposed to aerobic glycolysis.
Furthermore, with his experiments Dr Seyfried has been able to observe tumor regression using a form of ‘ketogenesis’ through dietary means.
He was able to utilize the knowledge that the human organism can be converted into a fat burner as opposed to a glucose burner. By adjusting the human diet from 0 or nearly 0 carbohydrate intake and ingesting more fat and protein the body will adapt to a ketogenic state.
 Ketogenesis occurs when glucose is very low and the hormone Glucagon is released from the pancreas to stabilize blood sugar. This stimulates the liver to take the fatty acid stores from the adipose tissue and produce water soluble ‘ketone bodies’ which act as fuel for the body and the brain, (this is a wonderful conversion ability that the body has, to combat starvation, when carbohydrates are not available ).
Ketogenesis occurs when glucose is very low and the hormone Glucagon is released from the pancreas to stabilize blood sugar. This stimulates the liver to take the fatty acid stores from the adipose tissue and produce water soluble ‘ketone bodies’ which act as fuel for the body and the brain, (this is a wonderful conversion ability that the body has, to combat starvation, when carbohydrates are not available ).
An example of this are the Eskimo who live purely on meat and fats from whale, walrus and fish. Except for berries that are found growing during the short summer season and the fermented carbohydrates from animal carcuses that are stored for future food supplys.
This Glucagon process is activated during our sleep cycle when we are not eating, and the liver takes over the blood sugar regulation from the pancreas insulin release process (this is why we lose weight during sleep because the insulin release is at 0, and if we maintain insulin at 0 for a while and consume 25% protein and 75% fat, a person can lose weight.
Most dietary regimens, such as low fat diets, etc, do not take into consideration the biological functioning of the human body and never work leaving people depressed and starving).
Our normal cells are able to use this new ketogenic fuel but according to Dr Seyfried the cancer cells cannot, so this effectively arrests the growth of the tumor cell proliferation (it kills some cancer cells, inhibits growth and reduces the tumor size).
This is disputable however, as explained in the next section.
The brain loves to burn fat the same way as the liver loves Kale. This is why coconut fat, butter, cholesterol is so therapeutic for the brain and preventative toward Alzheimer’s.
My grandmother would fry her ‘Bubble and Squeak’ (that’s yesterday’s leftover brussel sprouts and roast potatoes, my family like everybody else had ration books so food was scarce) in Lard and eat lots of eggs, butter and fatty meat, when she was a mother in 1940 during the Blitz.
It’s interesting to note that Alzheimer’s disease was never seen in the population prior to 1942.
Bob Atkins- The Famous Diet Doctor
As explained above, Ketogenesis converts the body into a fat burner, and in the initial stages, Glucagon, which is stored sugar from previous intake of carbohydrates, is produced by the liver, but this fuel is limited to a 8-12 hour burn and then its depleted.
At this point the adipose tissue (fat tissue) begins releasing fatty acids into the bloodstream and taken up by our cells to produce Acetyl Coenzyme A to feed the citric acid (Krebs) energy cycle.
While the body is in Ketosis, sugar is very limited and since the cancer cells are deprived access to glucose, and their energy process has decoupled from the Kreb cycle and electron transport the cancer cells have no means to survive.
Dr. Bob Atkins made a fortune ($300 million) from his famous ‘Atkins diet’ which was a version of the Ketogenic diet, and after his great success with the diet book (selling 100,000 copies/week at one point), he decided to set up a Cancer unit in 1987 and use his diet to treat cancer. After a while he observed that cancer patients were not improving so he eventually closed the unit down.
So it is doubtful that Ketogenesis is an efficient anticancer regimen.
The Inuit/Eskimo Diet
It is thought that the Inuit/Eskimo diet consisting of just fat and meat from consuming whale, seal, Caribou, walrus and fish was the perfect diet, since they had no reported chronic disease as Vilhjalmur Stefansson (1879-1962), a Canadian explorer and ethnologist reported, having lived with them for a few years. Apart from enlarged livers and excessive uric acid that the body uses to purge waste products from the Gluconeogenesis process in the liver, they appeared perfectly healthy.
Furthermore, it’s believed that their diet was a pure form of ketogenesis, however, multiple studies have shown this not to be the case. The Inuit preserve seals and birds to eat later, but during the preservation process proteins ferment into carbohydrates, and other marine animal like seal, that the Inuit consume, contain significant glycogen stores (8-30% carbohydrate) that the animals develop in order to survive oxygen depleted water depths. Strangely enough, despite their perceived good health, actual evidence has shown a high prevalence of cardiovascular abnormality.
Dr. Mcdougall a doctor in the U.S. and author (famous for shedding light on Multiple sclerosis with his association with Dr. Swank) informs us that the Eskimos derive their carbohydrate intake from plants, including berries, seaweed and roots, 2 months of the year during summer, as well as glycogen from the muscles and liver of the animals they consume.
A magazine article published in 1987 reported that 2 Eskimo women (one in her 20s, the other in her 40s) that had been frozen for 500 years were examined and found to have severe osteoporosis and atherosclerosis.
This would make sense since Dr McDougall states that because animal muscle contains very little calcium, the average daily intake for the Eskimo is 120 mg/day (1000 mg/day is the Recommended Daily Allowance).
Conclusion
So it turns out that some patients, who had their cancer regressed by the ketogenic diet were also receiving either chemotherapy and/or radiation simultaneously with the diet. Since Dr. Atkins was unsuccessful with his version of the ketogenic diet and cancer thrives in an anaerobic fermentation environment… Where does that leave us?
We are also now aware that 95% of conventional treatment for cancer is ineffective, except to extend people’s lives a little and even curative for initial stage blood cancers that may or may not return.
However, recently, scientists have discovered the biological root of cancer which is the stem cell. Up until recently these very poisonous treatments targeted the mature tumors and left the root cause in place only for it regrow from the undamaged stem cells.
How many times have you heard the story that my cancer has returned…IT NEVER LEFT
Finally, nobody ever mentions the immune system, the very system that regulates apoptosis (normal cell death) and kills many cancer cells daily (NKC – Natural Killer Cells) that inject the cancer cell with Hydrogen Peroxide to destroy it. Conventional medicine always wants to suppress the immune system and not harness its natural ability..I ask the question again..
WHO IS DRIVING THE BUS…US OR CANCER?

Alan: “I’m Alan Lombardo: stage 3 lymphoma. Pleased to meet you”.
Mitch: “Mitch Barnett, metastatic prostate cancer”.
Adam: “Oh, I’m Adam Lerner, schwannoma neurofibrosarcoma”.
Quote from the movie 50/50
References/Acknowledgments
- History of cancer (Article 2015) Nigel Hawkes
- Interferon Cancer research UK website
- Interferon Wikipedia
- What is the distinction between Chemokines,cytokines,interferons and Interleukins Biology website
- $89 million awarded to family who sued HMO (Article Dec 1993 NY Times) Erik Eckholm
- 2 endogenous anti-angiogenic inhibitors Endostatin, Angiostatin demonstrate biplasmic cures in their anti-tumor profiles ( NCBI 2011) K.Javaherian, T.Lee, R.Sjin, G.Pavru,L.Hlatky
- Endostatin Wikipedia
- Judah Folkman dies at 74 (Article Jan 2008 Harvard Gazette ) Robert Cooke
- Phase II Study of recombinant human endostatin in patients with advanced neuroendocrine tumors (NCBI 2006)
- Dr Gonzalez dismantles the Ketogenic diet (Article 2013) Dr Nicholas Gonzalez
- Citric acid cycle Khan Academy website
- Cancer: A Metabolic Disease With Metabolic Solutions Utube video Dr Thomas Seyfried
- Inheritance of traits by offspring follows preictable rules Scitable website
- What does glucagon do ? Hormone health network website
- Inuit diet Wikipedia
- Extreme nutrition : The diet of eskimos ( Vol 14, issue 4) Dr McDougall’s Health and medical website
Author: Eric Malouin